

Guidelines vs Actual Management of Skin and Soft Tissue Infections in the Emergency Department
- PMID: 29354655
- PMCID: PMC5767964
- DOI: 10.1093/ofid/ofx188
Guidelines vs Actual Management of Skin and Soft Tissue Infections in the Emergency Department
Abstract
Background: Infections of skin and soft tissue (SSTI) commonly cause visits to hospital emergency departments (EDs). The Infectious Diseases Society of America (IDSA) has published guidelines for the management of SSTI, but it is unclear how closely these guidelines are followed in practice.
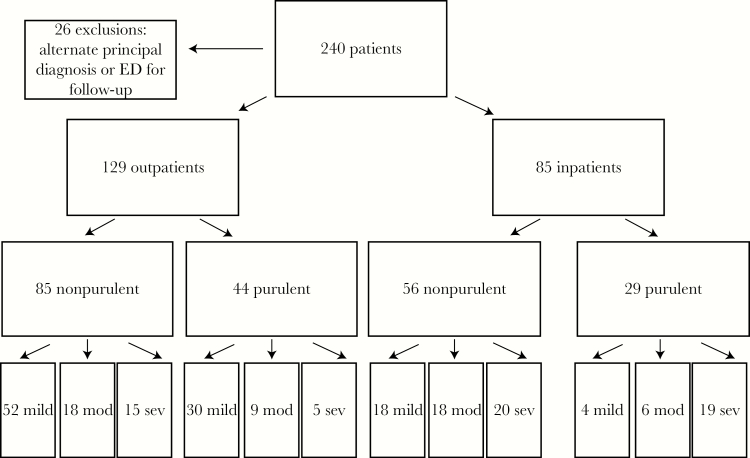
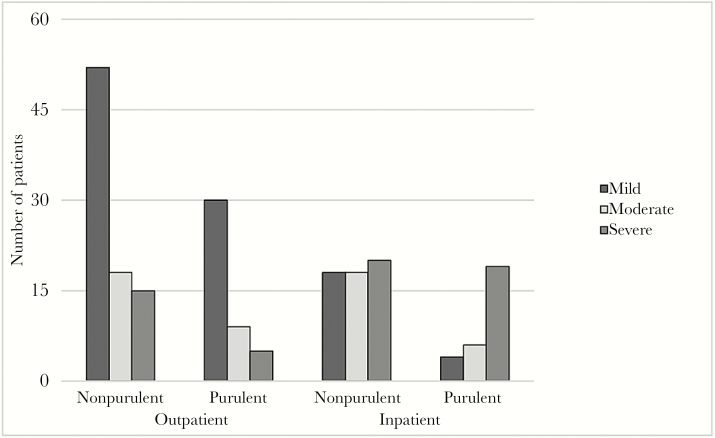
Methods: We reviewed records of patients seen in the ED at a large tertiary care hospital to determine guidelines adherence in 4 important areas: the decision to hospitalize, choice of antibiotics, incision and drainage (I&D) of abscesses, and submission of specimens for culture.
Results: The decision to hospitalize did not comply with guidelines in 19.6% of cases. Nonrecommended antibiotics were begun in the ED in 71% of patients with nonpurulent infections and 68.4% of patients with purulent infections. Abscesses of mild severity were almost always treated with antibiotics, and I&D was often not done (both against recommendations). Blood cultures were done (against recommendations) in 29% of patients with mild-severity cellulitis. Abscess drainage was almost always sent for culture (recommendations neither favor nor oppose). Overall, treatment fully complied with guidelines in 20.1% of cases.
Conclusions: Our results show a striking lack of concordance with IDSA guidelines in the ED management of SSTI. Social factors may account for discordant decisions regarding site of care. Use of trimethoprim/sulfamethoxazole (TMP/SMX) in cellulitis was the most common source of discordance; this practice is supported by some medical literature. Excess antibiotics were often used in cellulitis and after I&D of simple abscesses, opposing antibiotic stewardship. Ongoing education of ED doctors and continued review of published guidelines are needed.
Keywords: abscess; antibiotic stewardship; cellulitis; skin and soft tissue infection.
Figures
References
-
- Pallin DJ, Egan DJ, Pelletier AJ et al. Increased US emergency department visits for skin and soft tissue infections, and changes in antibiotic choices, during the emergence of community-associated methicillin-resistant Staphylococcus aureus. Ann Emerg Med 2008; 51:291–8. - PubMed
-
- Moran GJ, Krishnadasan A, Gorwitz RJ et al. ; EMERGEncy ID Net Study Group. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med 2006; 355:666–74. - PubMed
-
- Stevens DL, Bisno AL, Chambers HF et al. ; Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of skin and soft-tissue infections. Clin Infect Dis 2005; 41:1373–406. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
