

The Effect of Shorter Treatment Regimens for Hepatitis C on Population Health and Under Fixed Budgets
- PMID: 29354660
- PMCID: PMC5767946
- DOI: 10.1093/ofid/ofx267
The Effect of Shorter Treatment Regimens for Hepatitis C on Population Health and Under Fixed Budgets
Abstract
Background: Direct acting antiviral hepatitis C virus (HCV) therapies are highly effective but costly. Wider adoption of an 8-week ledipasvir/sofosbuvir treatment regimen could result in significant savings, but may be less efficacious compared with a 12-week regimen. We evaluated outcomes under a constrained budget and cost-effectiveness of 8 vs 12 weeks of therapy in treatment-naïve, noncirrhotic, genotype 1 HCV-infected black and nonblack individuals and considered scenarios of IL28B and NS5A resistance testing to determine treatment duration in sensitivity analyses.
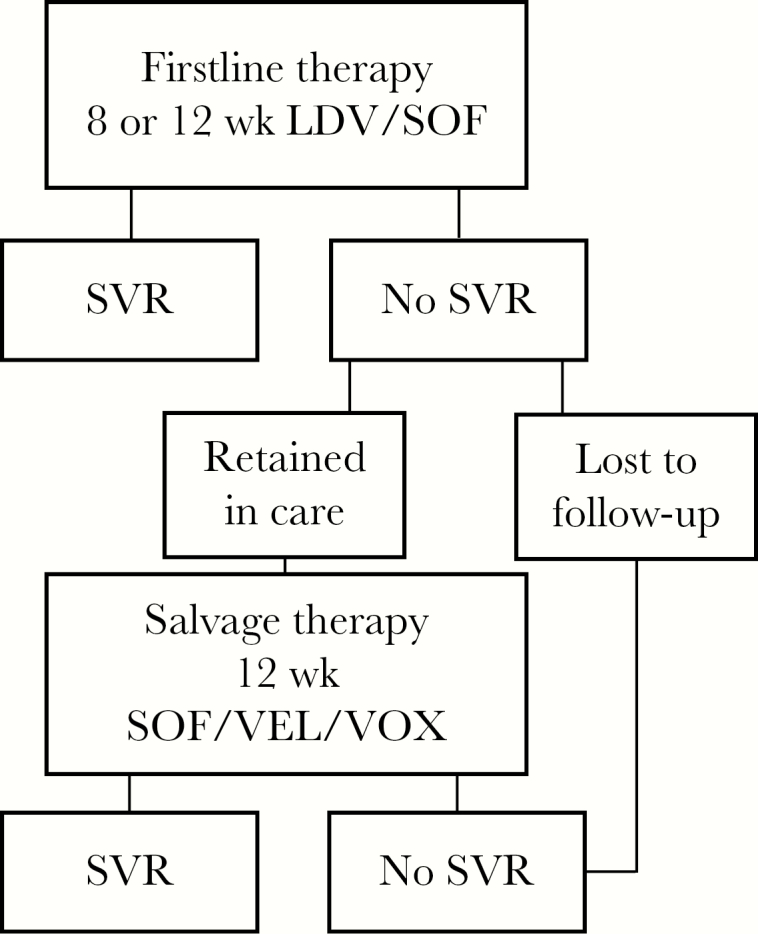
Methods: We developed a decision tree to use in conjunction with Monte Carlo simulation to investigate the cost-effectiveness of recommended treatment durations and the population health effect of these strategies given a constrained budget. Outcomes included the total number of individuals treated and attaining sustained virologic response (SVR) given a constrained budget and incremental cost-effectiveness ratios.
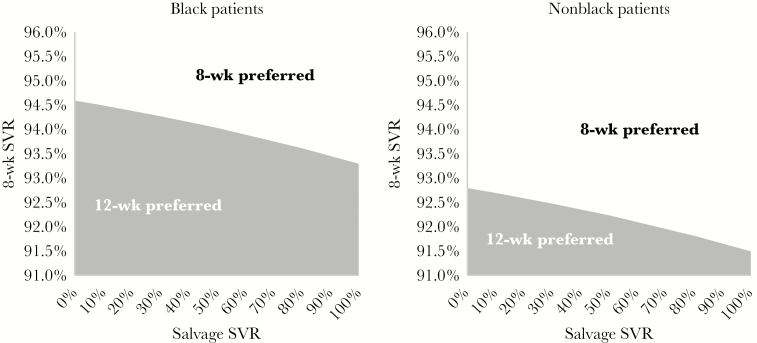
Results: We found that treating eligible (treatment-naïve, noncirrhotic, HCV-RNA <6 million copies) individuals with 8 weeks rather than 12 weeks of therapy was cost-effective and allowed for 50% more individuals to attain SVR given a constrained budget among both black and nonblack individuals, and our results suggested that NS5A resistance testing is cost-effective.
Conclusions: Eight-week therapy provides good value, and wider adoption of shorter treatment could allow more individuals to attain SVR on the population level given a constrained budget. This analysis provides an evidence base to justify movement of the 8-week regimen to the preferred regimen list for appropriate patients in the HCV treatment guidelines and suggests expanding that recommendation to black patients in settings where cost and relapse trade-offs are considered.
Keywords: IL28B; NS5A; budget impact; cost-effectiveness.
Figures
References
-
- Micromedex Solutions. Drug Topics Red Book Online Available at: http://www.micromedexsolutions.com. Accessed 13 September 2017.
-
- Barua S, Greenwald R, Grebely J et al. Restrictions for medicaid reimbursement of sofosbuvir for the treatment of hepatitis C virus infection in the United States. Ann Intern Med 2015; 163:215–23. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
