

Baseline and Serial Brain Natriuretic Peptide Level Predicts 5-Year Overall Survival in Patients With Pulmonary Arterial Hypertension: Data From the REVEAL Registry
- PMID: 29355551
- PMCID: PMC6859253
- DOI: 10.1016/j.chest.2018.01.009
Baseline and Serial Brain Natriuretic Peptide Level Predicts 5-Year Overall Survival in Patients With Pulmonary Arterial Hypertension: Data From the REVEAL Registry
Abstract
Background: Plasma brain natriuretic peptide (BNP) level is a prognostic biomarker in pulmonary arterial hypertension (PAH). Its impact on long-term overall survival (OS) was investigated in the Registry to Evaluate Early and Long-term Pulmonary Arterial Hypertension Disease Management (REVEAL), a 5-year observational, multicenter, US registry of patients with PAH.
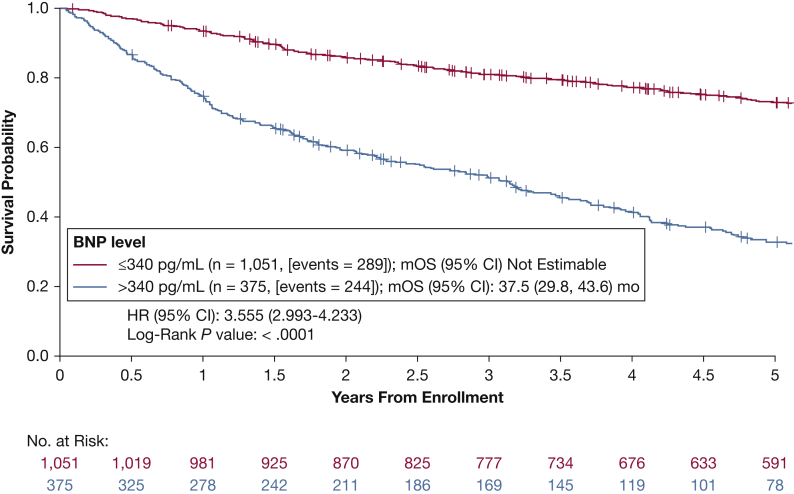
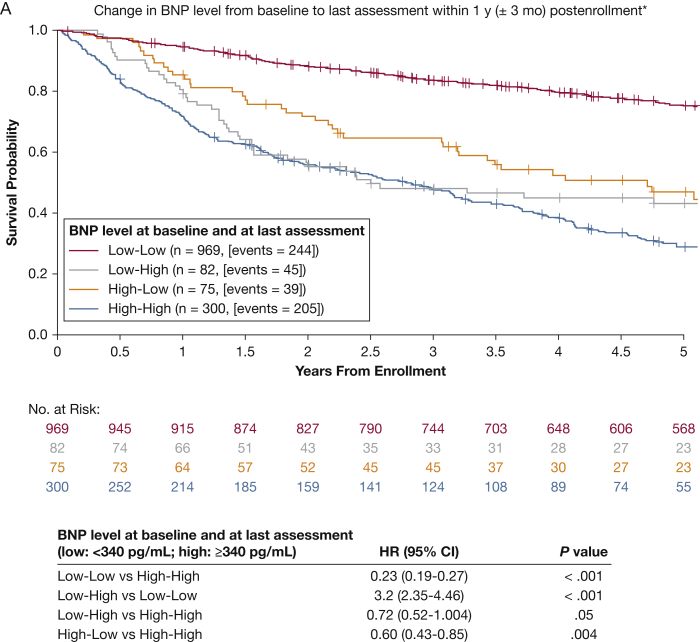
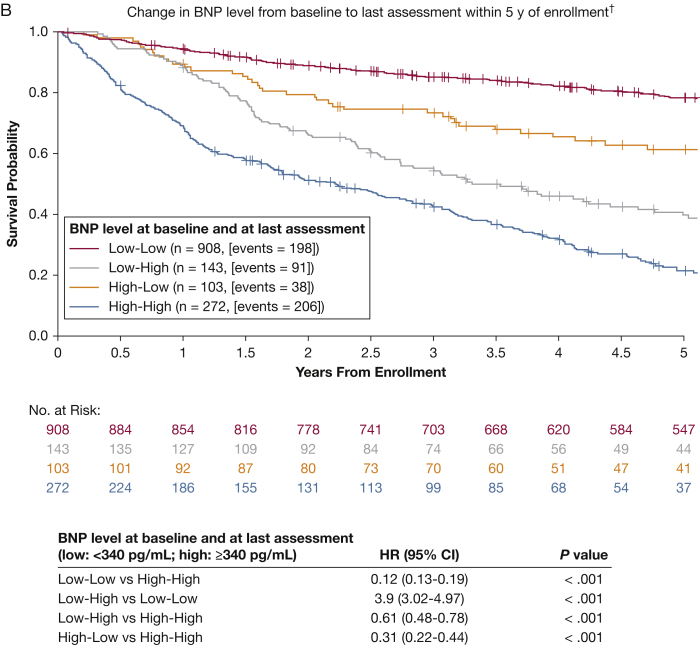
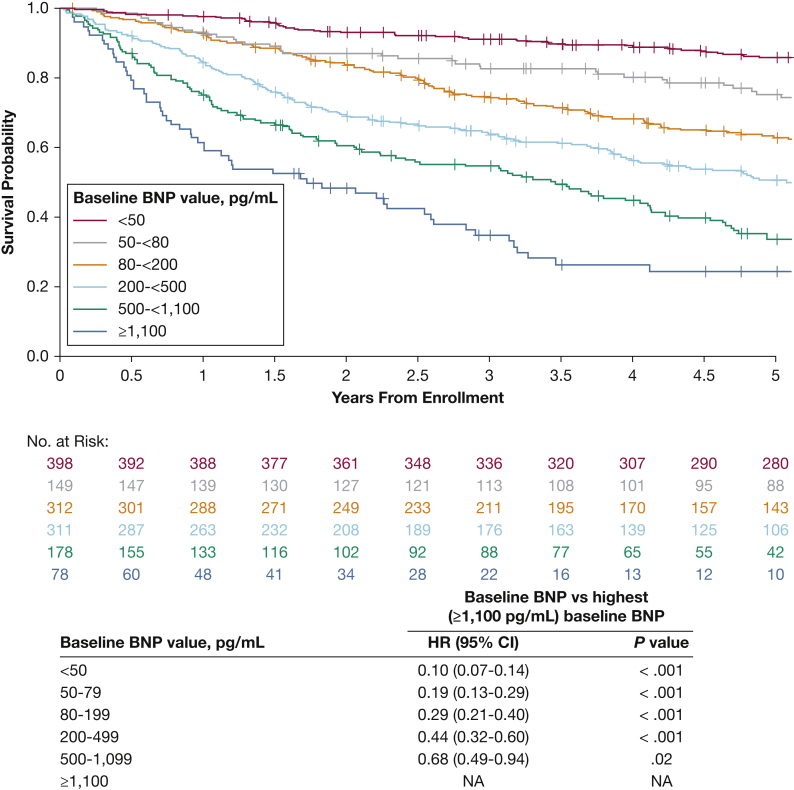
Methods: Patients were ≥ 18 years of age, met right heart catheterization criteria at rest, had World Health Organization group I PAH, and had BNP measurement at enrollment. Optimal BNP threshold was obtained via receiver operating characteristic curve analysis. OS was compared in patients with low (≤ 340 pg/mL) vs high (> 340 pg/mL) BNP at baseline; changes between baseline and last assessment were also examined. Patients were categorized based on baseline (low or high) and follow-up (low or high) BNP values; hazard ratios (HRs) for OS were estimated and compared using Cox regression.
Results: Overall, 1,426 patients were analyzed. Mortality risk was significantly higher in patients with baseline high vs low BNP (HR, 3.6; 95% CI, 3.0-4.2). BNP change analysis at ≤ 1 year postenrollment demonstrated that the low-low group had the lowest and the high-high group had the highest 5-year mortality risk (HR, 0.23; 95% CI, 0.19-0.27). Changes in BNP score also correlated with change of risk of death.
Conclusions: Baseline BNP threshold of 340 pg/mL strongly predicted survival up to 5 years in patients with PAH. A BNP reduction at 1 year since enrollment was associated with decreased mortality risk, whereas an increase in BNP at 1 year was associated with an increased mortality risk, supporting BNP as a surrogate marker of PAH survival.
Keywords: biomarkers; brain natriuretic peptide; mortality; pulmonary arterial hypertension; survival.
Copyright © 2018 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Response.Chest. 2018 Nov;154(5):1262-1264. doi: 10.1016/j.chest.2018.07.033. Chest. 2018. PMID: 30409362 No abstract available.
-
Untangling BNP and BMI: Does Obesity Limit the Predictive Capability of BNP in PAH?Chest. 2018 Nov;154(5):1262. doi: 10.1016/j.chest.2018.04.049. Chest. 2018. PMID: 30409363 No abstract available.
References
-
- Simonneau G., Gatzoulis M.A., Adatia I. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62(25):D34–D41. - PubMed
-
- Galiè N., Humbert M., Vachiery J.L. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT) Eur Respir J. 2015;46(4):903–975. - PubMed
-
- Humbert M., Sitbon O., Chaouat A. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173(9):1023–1030. - PubMed
-
- McGoon M.D., Benza R.L., Escribano-Subias P. Pulmonary arterial hypertension: epidemiology and registries. J Am Coll Cardiol. 2013;62(25):D51–D59. - PubMed
-
- Awdish R., Cajigas H. Definition, epidemiology and registries of pulmonary hypertension. Heart Fail Rev. 2016;21(3):223–228. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
