

Functional Trajectories Before and After Major Surgery in Older Adults
- PMID: 29356710
- PMCID: PMC6521949
- DOI: 10.1097/SLA.0000000000002659
Functional Trajectories Before and After Major Surgery in Older Adults
Erratum in
-
Functional Trajectories Before and After Major Surgery in Older Adults: Erratum.Ann Surg. 2019 Apr;269(4):e57. doi: 10.1097/SLA.0000000000003230. Ann Surg. 2019. PMID: 30845018 No abstract available.
Abstract
Objectives: We hypothesized that distinct sets of functional trajectories can be identified in the year before and after major surgery, with unique transition probabilities from pre to postsurgical functional trajectories, and that outcomes would be better among participants undergoing elective versus nonelective surgery.
Background: Major surgery is common and can be highly morbid in older persons. The relationship between the course of disability (ie, functional trajectory) before and after surgery in older adults has not been well-studied for most operations.
Methods: Prospective cohort study of 754 community-living persons 70 years or older. The analytic sample included 250 participants who underwent their first major surgery during the study period.
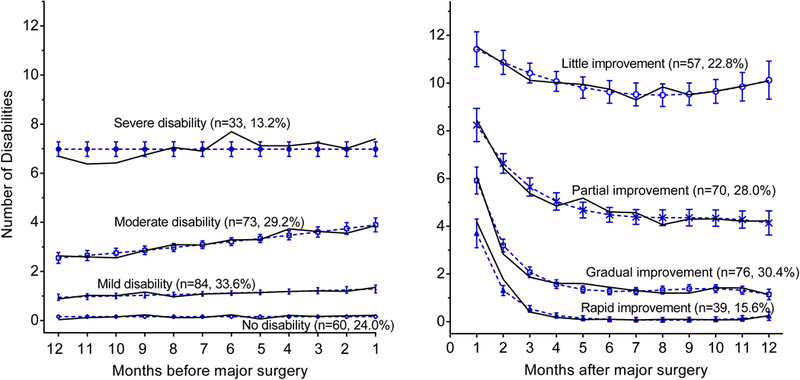
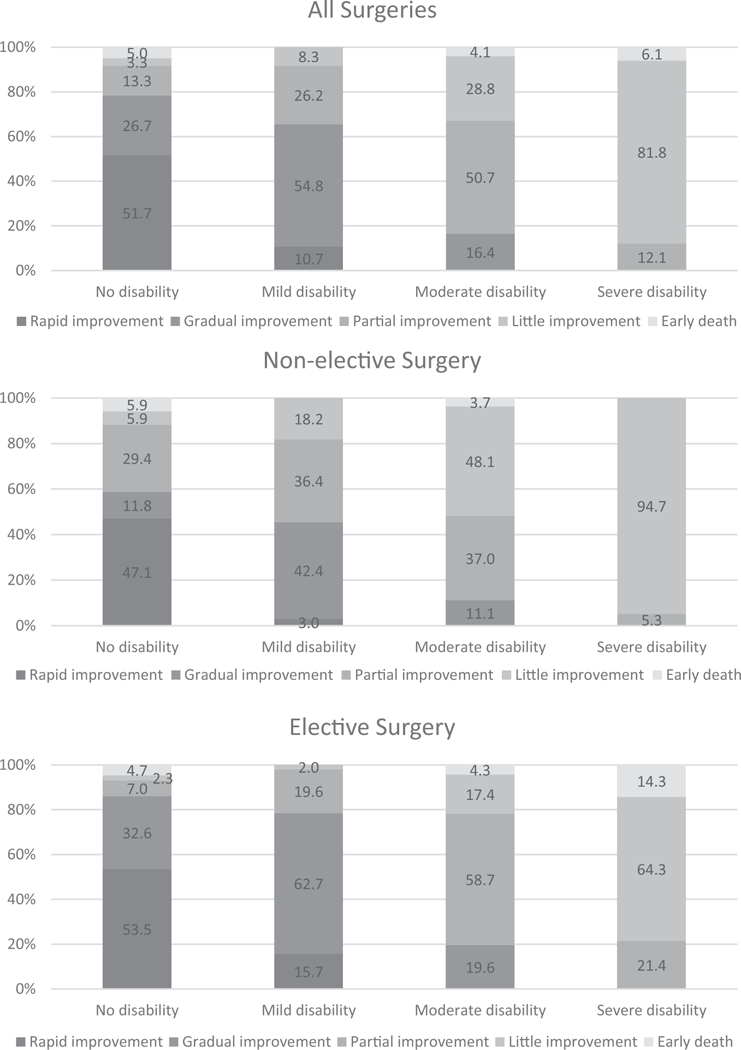
Results: Before surgery, 4 functional trajectories were identified: no disability (n = 60, 24.0%), and mild (n = 84, 33.6%), moderate (n = 73, 29.2%), and severe (n = 33, 13.2%) disability. After surgery, 4 functional trajectories were identified: rapid (n = 39, 15.6%), gradual (n = 76, 30.4%), partial (n = 70, 28.0%), and little (n = 57, 22.8%) improvement. Rapid improvement was seen for n = 31 (51.7%) participants with no disability before surgery, but was uncommon among those with mild disability (n = 8, 9.5%) and was not observed in the moderate and severe trajectory groups. For participants with mild to moderate disability before surgery, gradual improvement (n = 46, 54.8%) and partial improvement (n = 36, 49.3%) were most common. Most participants with severe disability (n = 27, 81.8%) before surgery exhibited little improvement. Outcomes were better for participants undergoing elective versus nonelective surgery.
Conclusions: Functional prognosis in the year after major surgery is highly dependent on premorbid function.
Conflict of interest statement
Conflicts of interest: Dr Gill is the recipient of an Academic Leadership Award (K07AG043587) from the National Institute on Aging. The organizations funding this study had no role in the design or conduct of the study; in the collection, management, analysis, or interpretation of the data; or in the preparation, review, or approval of the manuscript. The other authors report no conflicts of interest.
Figures
Comment in
-
Function: An Essential Postoperative Outcome for Older Adults.Ann Surg. 2018 Dec;268(6):918-919. doi: 10.1097/SLA.0000000000002866. Ann Surg. 2018. PMID: 29916873 No abstract available.
References
-
- Older Americans 2016: Key Indicators of Well-Being. In Statistics FIFoA-R, ed. Washington, DC: U.S. Government Printing Office; 2016.
-
- Elixhauser A, Andrews RM. Profile of inpatient operating room procedures in US hospitals in 2007. Arch Surg. 2010;145:1201–1208. - PubMed
-
- Rosenthal RA, Zenilman ME, Katlic MR. Principles and Practice of Geriatric Surgery. New York: Springer; 2011.
-
- McKinlay JB, Crawford SL, Tennstedt SL. The everyday impacts of providing informal care to dependent elders and their consequences for the care recipients. J Aging Health. 1995;7:497–528. - PubMed
-
- Schulz R, Beach SR. Caregiving as a risk factor for mortality: the Caregiver Health Effects Study. JAMA. 1999;282:2215–2219. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
