

Management of spinal infection: a review of the literature
- PMID: 29356895
- PMCID: PMC5807463
- DOI: 10.1007/s00701-018-3467-2
Management of spinal infection: a review of the literature
Abstract
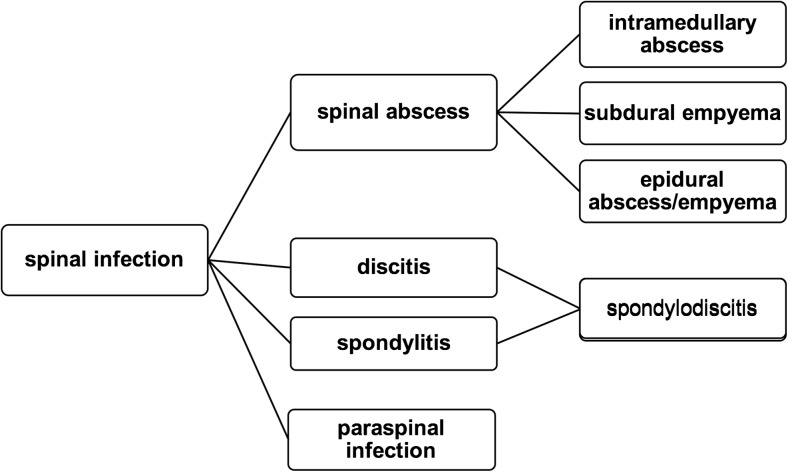
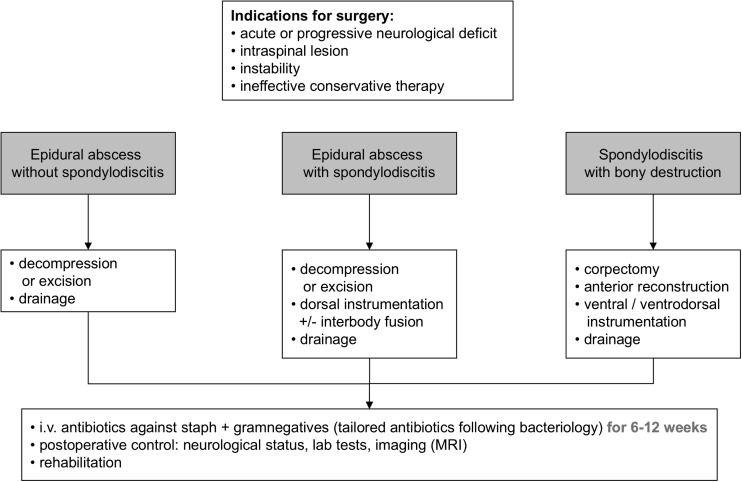
Spinal infection (SI) is defined as an infectious disease affecting the vertebral body, the intervertebral disc, and/or adjacent paraspinal tissue and represents 2-7% of all musculoskeletal infections. There are numerous factors, which may facilitate the development of SI including not only advanced patient age and comorbidities but also spinal surgery. Due to the low specificity of signs, the delay in diagnosis of SI remains an important issue and poor outcome is frequently seen. Diagnosis should always be supported by clinical, laboratory, and imaging findings, magnetic resonance imaging (MRI) remaining the most reliable method. Management of SI depends on the location of the infection (i.e., intraspinal, intervertebral, paraspinal), on the disease progression, and of course on the patient's general condition, considering age and comorbidities. Conservative treatment mostly is reasonable in early stages with no or minor neurologic deficits and in case of severe comorbidities, which limit surgical options. Nevertheless, solely medical treatment often fails. Therefore, in case of doubt, surgical treatment should be considered. The final result in conservative as well as in surgical treatment always is bony fusion. Furthermore, both options require a concomitant antimicrobial therapy, initially applied intravenously and administered orally thereafter. The optimal duration of antibiotic therapy remains controversial, but should never undercut 6 weeks. Due to a heterogeneous and often comorbid patient population and the wide variety of treatment options, no generally applicable guidelines for SI exist and management remains a challenge. Thus, future prospective randomized trials are necessary to substantiate treatment strategies.
Keywords: Intramedullary abscess; Spinal epidural abscess; Spinal infection; Spondylodiscitis; Subdural empyema; Vertebral osteomyelitis.
Conflict of interest statement
Conflict of interest
CT receives speaker honoraria and grant research support from medical implant companies. All other authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
For this type of study, ethical approval is not required.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
