

Individualised treatment targets in patients with type-2 diabetes and hypertension
- PMID: 29357854
- PMCID: PMC5778654
- DOI: 10.1186/s12933-018-0661-8
Individualised treatment targets in patients with type-2 diabetes and hypertension
Abstract
Aim: Patients with type-2 diabetes mellitus (T2DM) are at high risk of cardiovascular events, accentuated in the presence of hypertension. At present, it is unclear to what extent the guidelines for the management of T2DM, advocating reduction in HbA1c levels to below target levels, are being adhered to in clinical practice.
Methods: DIALOGUE was a prospective, observational, non-interventional registry performed across multiple centres in Germany. Patients aged 18 years or older who had T2DM and hypertension for whom the treating physician considered blood glucose lowering medication as inadequate and/or not safe/tolerable and chose to add a further oral drug or switch drug treatment were included. Patients were assigned a treatment target HbA1c value (≤ 6.5% [strict]; > 6.5 to ≤ 7.0% [intermediate]; > 7.0 to ≤ 7.5% [lenient]).
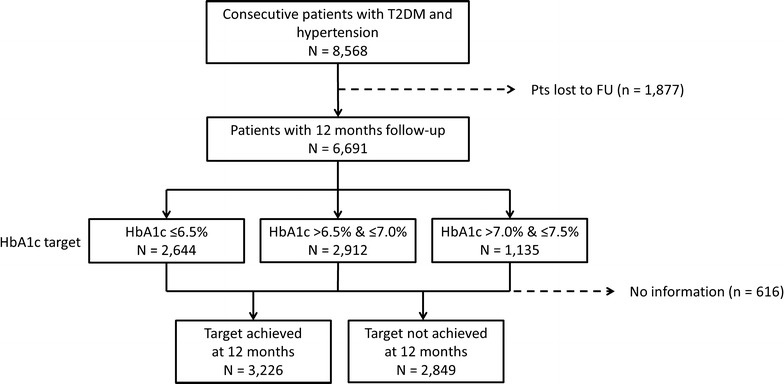
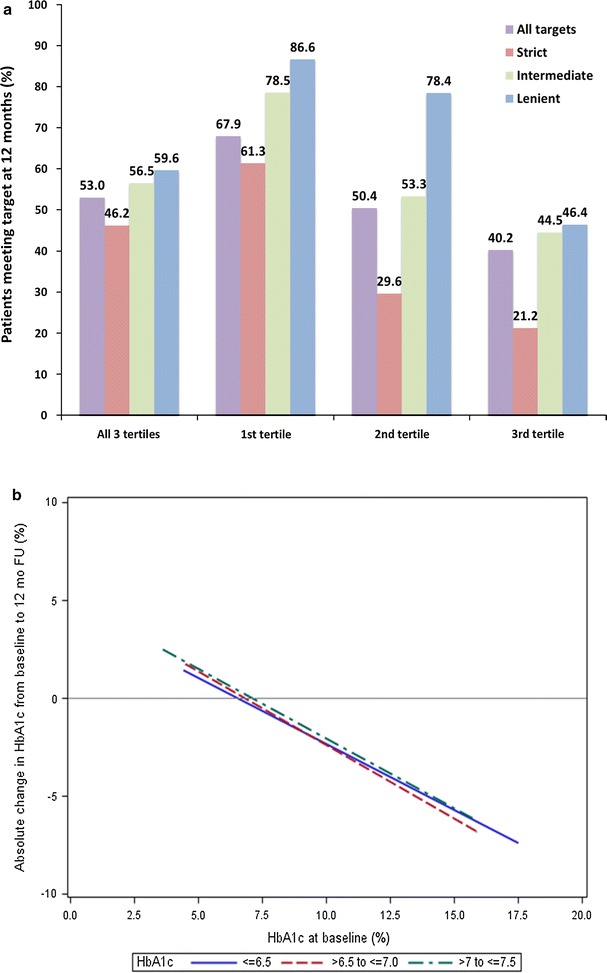
Results: 8568 patients with T2DM and hypertension were enrolled. 6691 (78.1%) had 12-month follow-up. Patients who were assigned a strict HbA1c treatment target (n = 2644) were younger, had shorter diabetes duration, and less comorbidity in comparison to those with intermediate (n = 2912) or lenient targets (n = 1135). Only 53.1% of patients achieved their HbA1c treatment target (46.2% [strict], 56.8% [intermediate], 59.4% [lenient]). There was little sign of treatment intensification for patients that had not achieved their HbA1c target.
Conclusions: Achievement of treatment targets was poor, leaving many patients with sub-optimal blood glucose levels. The apparent reluctance of physicians to intensify antidiabetic drug therapy is alarming, especially considering the evidence pointing to an association of hyperglycaemia and microvascular complications in patients with T2DM.
Keywords: Diabetes; Glucose; HbA1c; Hyperglycaemia; Hypertension; Individualised; Target.
Figures

References
-
- Adler AI, Stratton IM, Neil HA, Yudkin JS, Matthews DR, Cull CA, Wright AD, Turner RC, Holman RR. Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): Prospective Observational Study. BMJ. 2000;321(7258):412–419. doi: 10.1136/bmj.321.7258.412. - DOI - PMC - PubMed
-
- Fox CS, Golden SH, Anderson C, Bray GA, Burke LE, de Boer IH, Deedwania P, Eckel RH, Ershow AG, Fradkin J, Inzucchi SE, Kosiborod M, Nelson RG, Patel MJ, Pignone M, Quinn L, Schauer PR, Selvin E, Vafiadis DK. Update on prevention of cardiovascular disease in adults with type 2 diabetes mellitus in light of recent evidence: a Scientific Statement from the American Heart Association and the American Diabetes Association. Circulation. 2015;132(8):691–718. doi: 10.1161/CIR.0000000000000230. - DOI - PMC - PubMed
-
- Ruckert IM, Schunk M, Holle R, Schipf S, Volzke H, Kluttig A, Greiser KH, Berger K, Muller G, Ellert U, Neuhauser H, Rathmann W, Tamayo T, Moebus S, Andrich S, Meisinger C. Blood pressure and lipid management fall far short in persons with type 2 diabetes: results from the DIAB-CORE Consortium including six German population-based studies. Cardiovasc Diabetol. 2012;11:50. doi: 10.1186/1475-2840-11-50. - DOI - PMC - PubMed
-
- Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, Sherwin R, Zinman B. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2009;32(1):193–203. doi: 10.2337/dc08-9025. - DOI - PMC - PubMed
-
- American Diabetes Association Executive summary: standards of medical care in diabetes–2014. Diabetes Care. 2014;37(Suppl 1):S5–S13. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
