

Embedding weight management into safety-net pediatric primary care: randomized controlled trial
- PMID: 29357894
- PMCID: PMC5778780
- DOI: 10.1186/s12966-017-0639-z
Embedding weight management into safety-net pediatric primary care: randomized controlled trial
Abstract
Background: Implementing evidence-based recommendations for treating pediatric overweight and obesity is challenging in low-resource settings. We conducted a randomized controlled trial to evaluate the effects of implementing the American Academy of Pediatrics overweight/obesity recommendations using a Standard Care approach alone or with the addition of an enhanced program in a safety-net pediatric primary care setting (located in Bronx, New York, United States).
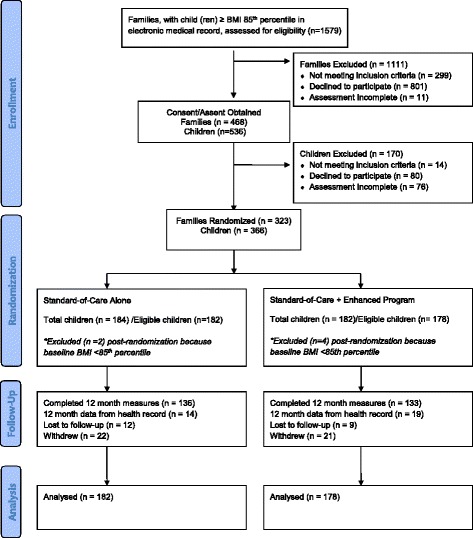
Methods: In a 12-month trial, families of children (age 7-12 years; body mass index ≥85th American percentile for age and sex; 74% self-identified as Hispanic/Latino; n = 360) were randomly assigned to receive Standard Care Alone or Standard Care + Enhanced Program. An English/Spanish bilingual staff provided the Standard Care Alone consisting of quarterly semi-structured pediatrician visits targeting family-based behavioral changes. The Standard Care + Enhanced Program was enriched with eight Skill-Building Core and monthly Post-Core Support sessions.
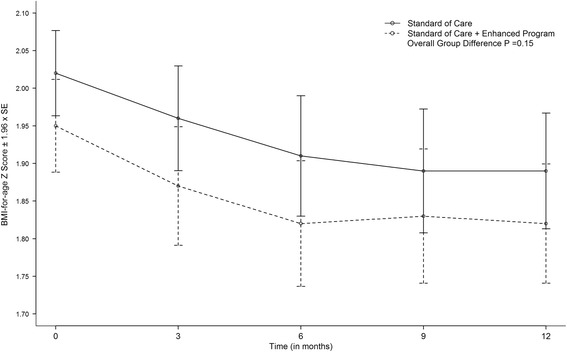
Results: The mean body mass index Z-score declined in both arms (P < 0.01) with no significant difference between the Standard Care Alone (0.12 kg [SE: 0.03]) and Standard Care + Enhanced Program (0.15 kg [SE: 0.03]) arm (P = 0.15). Compared to the Standard Care Alone, the Standard Care + Enhanced Program resulted in significantly greater improvements in total cholesterol (P = 0.05), low-density lipoprotein cholesterol (P = 0.04), aspartate aminotransferase (P = 0.02), and alanine transaminase (P = 0.03) concentrations.
Conclusions: Safety-net primary care settings can provide efficacious pediatric weight management services. Targeted family-based behavioral counseling helps overweight/obese children achieve a modest body mass index Z-score improvement. A more intensive lifestyle intervention program may improve some metabolic parameters.
Trial registration: ClinicalTrials.gov Identifier: NCT00851201 . Registered 23 February 2009.
Keywords: Family-based intervention; Safety net care; Weight management.
Conflict of interest statement
Ethics approval and consent to participate
All study procedures were approved by the Institutional Review Boards of the Albert Einstein College of Medicine and Tufts University. Written consent was obtained from all par-ent/guardian and assent was obtained from children entered into the study.
Consent for publication
Not applicable.
Competing interests
The authors have no conflict of interests to disclose, and the authors have no financial relationships relevant to this article to disclose.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
