

Symptom-Disease Pair Analysis of Diagnostic Error (SPADE): a conceptual framework and methodological approach for unearthing misdiagnosis-related harms using big data
- PMID: 29358313
- PMCID: PMC6049698
- DOI: 10.1136/bmjqs-2017-007032
Symptom-Disease Pair Analysis of Diagnostic Error (SPADE): a conceptual framework and methodological approach for unearthing misdiagnosis-related harms using big data
Abstract
Background: The public health burden associated with diagnostic errors is likely enormous, with some estimates suggesting millions of individuals are harmed each year in the USA, and presumably many more worldwide. According to the US National Academy of Medicine, improving diagnosis in healthcare is now considered 'a moral, professional, and public health imperative.' Unfortunately, well-established, valid and readily available operational measures of diagnostic performance and misdiagnosis-related harms are lacking, hampering progress. Existing methods often rely on judging errors through labour-intensive human reviews of medical records that are constrained by poor clinical documentation, low reliability and hindsight bias.
Methods: Key gaps in operational measurement might be filled via thoughtful statistical analysis of existing large clinical, billing, administrative claims or similar data sets. In this manuscript, we describe a method to quantify and monitor diagnostic errors using an approach we call 'Symptom-Disease Pair Analysis of Diagnostic Error' (SPADE).
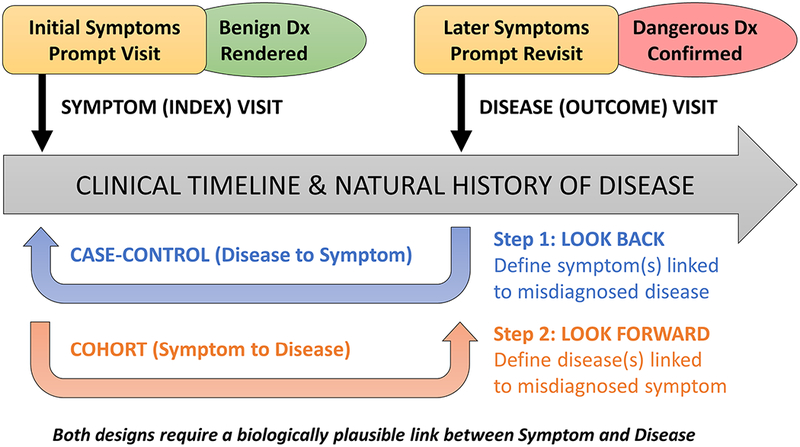
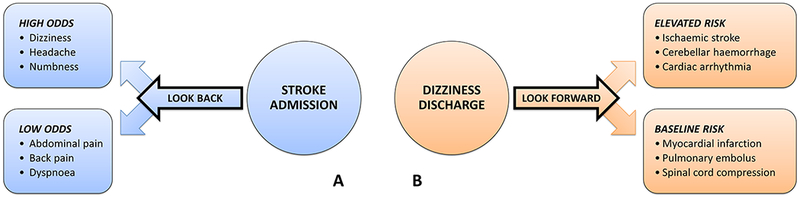
Results: We first offer a conceptual framework for establishing valid symptom-disease pairs illustrated using the well-known diagnostic error dyad of dizziness-stroke. We then describe analytical methods for both look-back (case-control) and look-forward (cohort) measures of diagnostic error and misdiagnosis-related harms using 'big data'. After discussing the strengths and limitations of the SPADE approach by comparing it to other strategies for detecting diagnostic errors, we identify the sources of validity and reliability that undergird our approach.
Conclusion: SPADE-derived metrics could eventually be used for operational diagnostic performance dashboards and national benchmarking. This approach has the potential to transform diagnostic quality and safety across a broad range of clinical problems and settings.
Keywords: diagnostic errors; epidemiology/diagnosis; outcome measures/methods; patient harm; process measures/methods; public health informatics/methods.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
The data of diagnostic error: big, large and small.BMJ Qual Saf. 2018 Jul;27(7):499-501. doi: 10.1136/bmjqs-2018-007917. Epub 2018 Mar 5. BMJ Qual Saf. 2018. PMID: 29507123 No abstract available.
References
-
- National Academies of Sciences, Engineering, and Medicine. Improving diagnosis in health care. Washington, DC: The National Academies Press, 2015.
-
- Newman-Toker DE. Diagnostic value: the economics of high-quality diagnosis and a value-based perspective on diagnostic innovation [lecture]. Modern Healthcare 3rd Annual Patient Safety & Quality Virtual Conference;2015 June 17;online e-conference.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous