

Disparities in spread and control of influenza in slums of Delhi: findings from an agent-based modelling study
- PMID: 29358419
- PMCID: PMC5780711
- DOI: 10.1136/bmjopen-2017-017353
Disparities in spread and control of influenza in slums of Delhi: findings from an agent-based modelling study
Abstract
Objectives: This research studies the role of slums in the spread and control of infectious diseases in the National Capital Territory of India, Delhi, using detailed social contact networks of its residents.
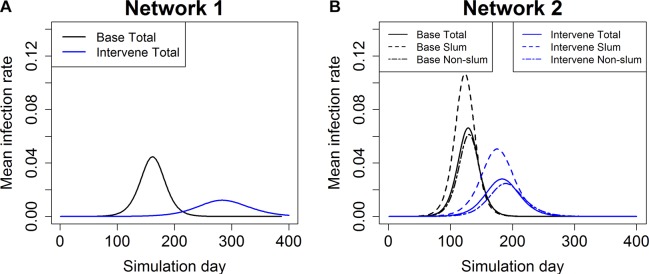
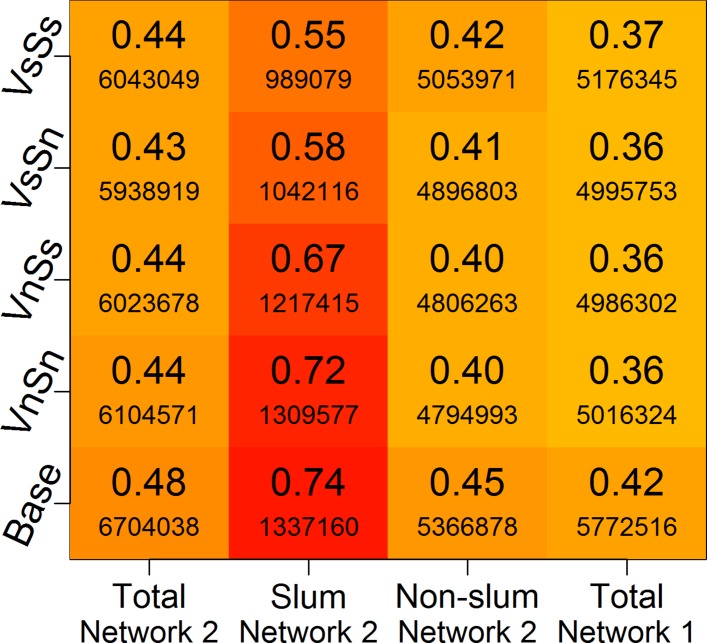
Methods: We use an agent-based model to study the spread of influenza in Delhi through person-to-person contact. Two different networks are used: one in which slum and non-slum regions are treated the same, and the other in which 298 slum zones are identified. In the second network, slum-specific demographics and activities are assigned to the individuals whose homes reside inside these zones. The main effects of integrating slums are that the network has more home-related contacts due to larger family sizes and more outside contacts due to more daily activities outside home. Various vaccination and social distancing interventions are applied to control the spread of influenza.
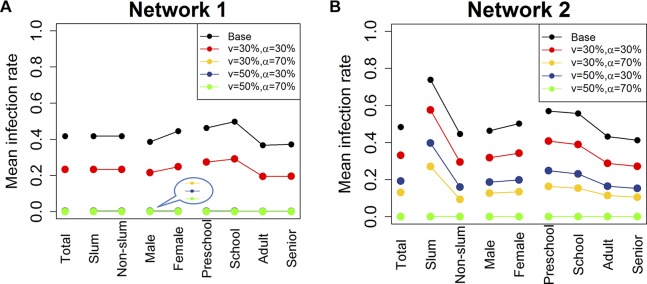
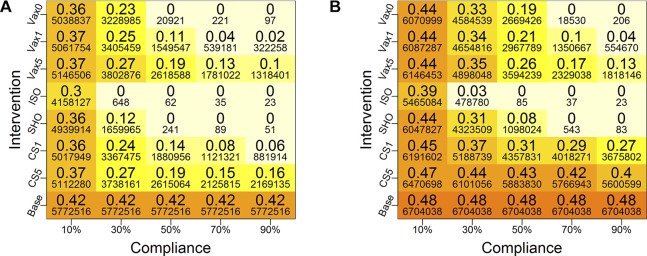
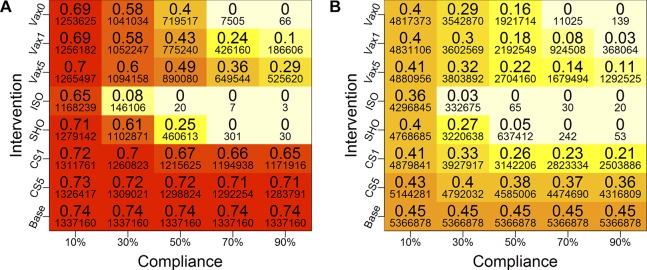
Results: Simulation-based results show that when slum attributes are ignored, the effectiveness of vaccination can be overestimated by 30%-55%, in terms of reducing the peak number of infections and the size of the epidemic, and in delaying the time to peak infection. The slum population sustains greater infection rates under all intervention scenarios in the network that treats slums differently. Vaccination strategy performs better than social distancing strategies in slums.
Conclusions: Unique characteristics of slums play a significant role in the spread of infectious diseases. Modelling slums and estimating their impact on epidemics will help policy makers and regulators more accurately prioritise allocation of scarce medical resources and implement public health policies.
Keywords: delhi; epidemic; interventions; slum population; synthetic social contact network.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Chandra N. Influenza viruses circulate in Delhi throughout the year, 2012. http://indiatoday.intoday.in/story/influenza-viruses-circulate-in-delhi-....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical