

Cost-effectiveness of an internet-based perioperative care programme to enhance postoperative recovery in gynaecological patients: economic evaluation alongside a stepped-wedge cluster-randomised trial
- PMID: 29358423
- PMCID: PMC5780709
- DOI: 10.1136/bmjopen-2017-017782
Cost-effectiveness of an internet-based perioperative care programme to enhance postoperative recovery in gynaecological patients: economic evaluation alongside a stepped-wedge cluster-randomised trial
Abstract
Objectives: To evaluate the cost-effectiveness and cost-utility of an internet-based perioperative care programme compared with usual care for gynaecological patients.
Design: Economic evaluation from a societal perspective alongside a stepped-wedge cluster-randomised controlled trial with 12 months of follow-up.
Setting: Secondary care, nine hospitals in the Netherlands, 2011-2014.
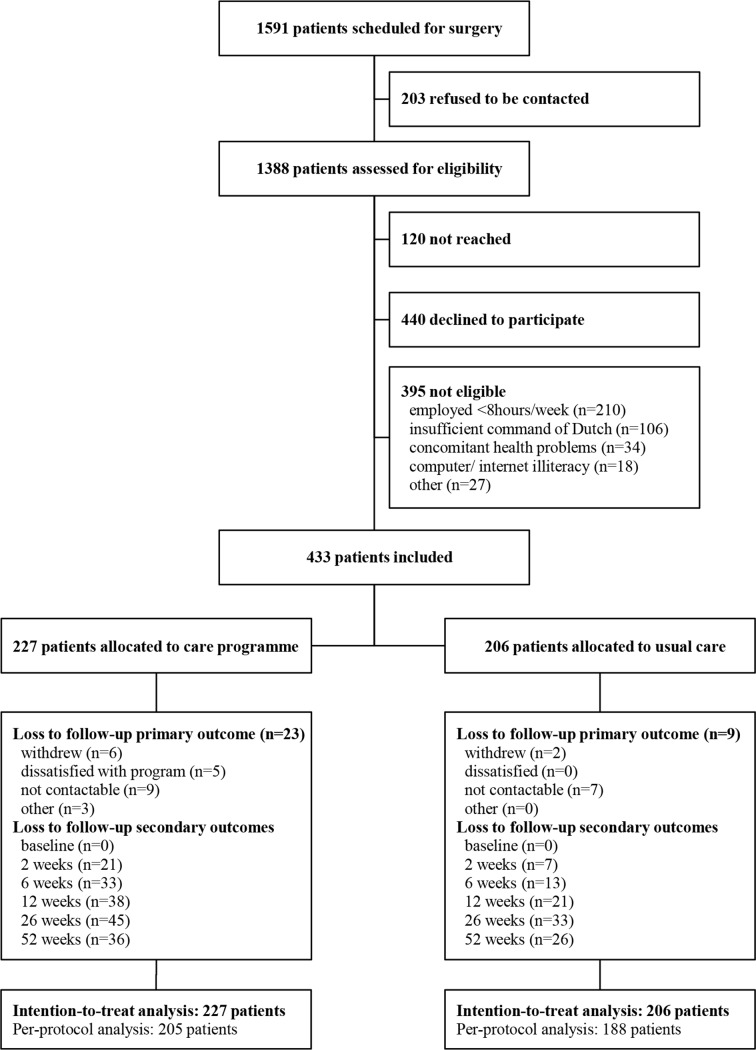
Participants: 433 employed women aged 18-65 years scheduled for a hysterectomy and/or laparoscopic adnexal surgery.
Intervention: The intervention comprised an internet-based care programme aimed at improving convalescence and preventing delayed return to work (RTW) following gynaecological surgery and was sequentially rolled out. Depending on the implementation phase of their hospital, patients were allocated to usual care (n=206) or to the intervention (n=227).
Main outcome measures: The primary outcome was duration until full sustainable RTW. Secondary outcomes were quality-adjusted life years (QALYs), health-related quality of life and recovery.
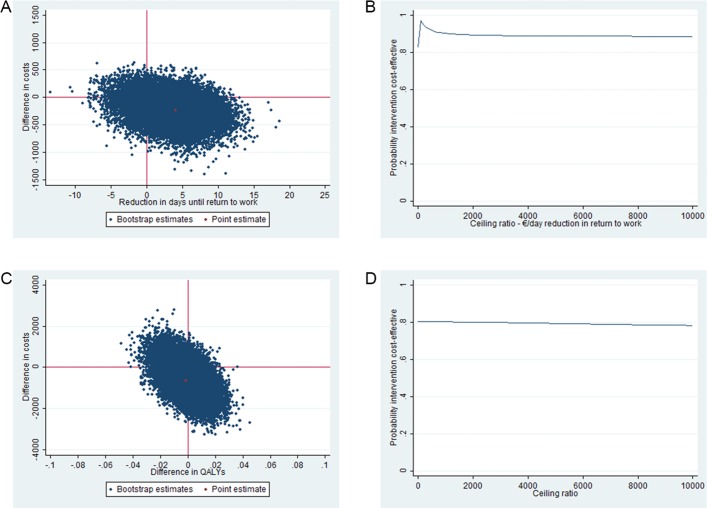
Results: At 12 months, there were no statistically significant differences in total societal costs (€-647; 95% CI €-2116 to €753) and duration until RTW (-4.1; 95% CI -10.8 to 2.6) between groups. The incremental cost-effectiveness ratio (ICER) for RTW was 56; each day earlier RTW in the intervention group was associated with cost savings of €56 compared with usual care. The probability of the intervention being cost-effective was 0.79 at a willingness-to-pay (WTP) of €0 per day earlier RTW, which increased to 0.97 at a WTP of €76 per day earlier RTW. The difference in QALYs gained over 12 months between the groups was clinically irrelevant resulting in a low probability of cost-effectiveness for QALYs.
Conclusions: Considering that on average the costs of a day of sickness absence are €230, the care programme is considered cost-effective in comparison with usual care for duration until sustainable RTW after gynaecological surgery for benign disease. Future research should indicate whether widespread implementation of this care programme has the potential to reduce societal costs associated with gynaecological surgery.
Trial registration number: NTR2933; Results.
Keywords: gynaecology; health economics; minimally invasive surgery; organisation of health services; telemedicine.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: JRA reports a chair in Insurance Medicine paid by the Dutch Social Security Agency, and he is a stockholder of Evalua. JAFH reports grants from Samsung, Gideon Richter and Celonova outside the submitted work. HAMB reports grants from Olympus and personal fees from Nordic Farma during the conduct of the study. JRA and JAFH are planning to set up a spin-off company concerning the implementation of a mobile application concerning the ikherstel intervention in the Netherlands.
Figures
Similar articles
-
Effectiveness of an internet-based perioperative care programme to enhance postoperative recovery in gynaecological patients: cluster controlled trial with randomised stepped-wedge implementation.BMJ Open. 2018 Jan 30;8(1):e017781. doi: 10.1136/bmjopen-2017-017781. BMJ Open. 2018. PMID: 29382673 Free PMC article. Clinical Trial.
-
A participatory supportive return to work program for workers without an employment contract, sick-listed due to a common mental disorder: an economic evaluation alongside a randomized controlled trial.BMC Public Health. 2017 Feb 2;17(1):162. doi: 10.1186/s12889-017-4079-0. BMC Public Health. 2017. PMID: 28152999 Free PMC article. Clinical Trial.
-
A personalised eHealth programme reduces the duration until return to work after gynaecological surgery: results of a multicentre randomised trial.BJOG. 2014 Aug;121(9):1127-35; discussion 1136. doi: 10.1111/1471-0528.12661. Epub 2014 Feb 11. BJOG. 2014. PMID: 24511914 Clinical Trial.
-
Evidence-informed decision about (de-)implementing return-to-work coordination to reduce sick leave: a case study.Health Res Policy Syst. 2022 Feb 14;20(1):19. doi: 10.1186/s12961-022-00823-4. Health Res Policy Syst. 2022. PMID: 35164766 Free PMC article. Review.
-
Cost effectiveness of guided Internet-based interventions for depression in comparison with control conditions: An individual-participant data meta-analysis.Depress Anxiety. 2018 Mar;35(3):209-219. doi: 10.1002/da.22714. Epub 2018 Jan 12. Depress Anxiety. 2018. PMID: 29329486 Free PMC article. Review.
Cited by
-
Observational retrospective study of UK national success, risks and costs for 319,105 IVF/ICSI and 30,669 IUI treatment cycles.BMJ Open. 2020 Mar 16;10(3):e034566. doi: 10.1136/bmjopen-2019-034566. BMJ Open. 2020. PMID: 32184314 Free PMC article.
-
How to analyze work productivity loss due to health problems in randomized controlled trials? A simulation study.BMC Med Res Methodol. 2021 Jun 24;21(1):130. doi: 10.1186/s12874-021-01330-w. BMC Med Res Methodol. 2021. PMID: 34162350 Free PMC article.
-
Strategies for facilitating the delivery of cluster randomized trials in hospitals: A study informed by the CFIR-ERIC matching tool.Clin Trials. 2021 Aug;18(4):398-407. doi: 10.1177/17407745211001504. Epub 2021 Apr 16. Clin Trials. 2021. PMID: 33863242 Free PMC article.
-
The development of multidisciplinary convalescence recommendations after childbirth: a modified Delphi study.AJOG Glob Rep. 2024 Oct 28;4(4):100411. doi: 10.1016/j.xagr.2024.100411. eCollection 2024 Nov. AJOG Glob Rep. 2024. PMID: 39634200 Free PMC article.
-
Recommendations for the Design and Delivery of Transitions-Focused Digital Health Interventions: Rapid Review.JMIR Aging. 2022 May 19;5(2):e35929. doi: 10.2196/35929. JMIR Aging. 2022. PMID: 35587874 Free PMC article. Review.
References
-
- Cox H. Recovery from gynaecological day surgery: are we underestimating the process. Ambul Surg 2003;10:114–21. 10.1016/S0966-6532(03)00007-6 - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical