

Intra-retinal Arterial Cannulation using a Microneedle for Central Retinal Artery Occlusion
- PMID: 29358594
- PMCID: PMC5778058
- DOI: 10.1038/s41598-018-19747-7
Intra-retinal Arterial Cannulation using a Microneedle for Central Retinal Artery Occlusion
Abstract
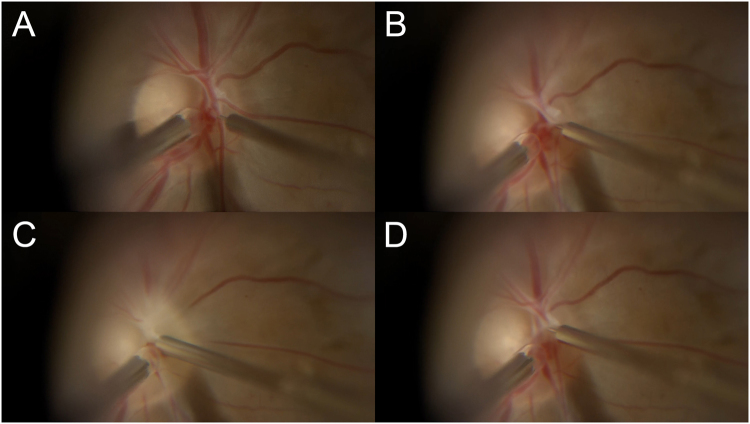
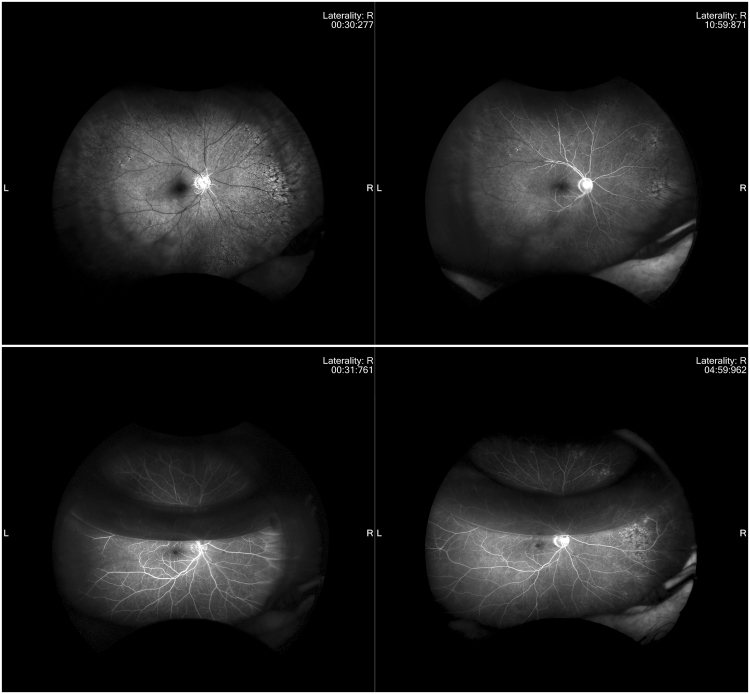
Central retinal artery occlusion (CRAO) is a severe disease, often causing blindness. We evaluated the efficacy and safety of a surgical procedure for the treatment of acute CRAO in which retinal arterial cannulation with tissue plasminogen activator (tPA) is performed. The surgical procedure consisted of vitrectomy followed by cannulation of the central retinal artery and injection of tPA (200 μg) using a 47-gauge microneedle. Thirteen CRAO patients were treated within 48 hours of the onset of symptoms. The central retinal artery of all 13 eyes was successfully cannulated. The mean interval between the onset of symptoms and surgery was 38.7 hours. The results for all 13 eyes treated showed a statistically significant improvement in mean visual acuity between before and one month after treatment (-1.60 vs. -0.82 logarithmic values for minimum angle resolution (LogMAR), p = 0.0021). Fluorescein angiography showed complete reperfusion and incomplete reperfusion in 10 eyes and 3 eyes, respectively. Recently developed surgical instruments have made retinal-arterial cannulation feasible. Intra-retinal-arterial cannulation has potential as a method of improving visual function and microcirculation in eyes affected by CRAO.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
Updated cannulation technique for tissue plasminogen activator injection into peripapillary retinal vein for central retinal vein occlusion.Acta Ophthalmol. 2015 Dec;93(8):739-44. doi: 10.1111/aos.12830. Epub 2015 Aug 27. Acta Ophthalmol. 2015. PMID: 26310993
-
Efficacy and safety of intra-arterial thrombolysis in central retinal artery occlusion.Invest Ophthalmol Vis Sci. 2013 Nov 21;54(12):7746-55. doi: 10.1167/iovs.13-12952. Invest Ophthalmol Vis Sci. 2013. PMID: 24176901
-
Endovascular Management of Central Retinal Arterial Occlusion.Vasc Endovascular Surg. 2016 Nov;50(8):579-581. doi: 10.1177/1538574416682158. Vasc Endovascular Surg. 2016. PMID: 28081693
-
Network Meta-Analysis of Different Thrombolytic Strategies for the Treatment of Central Retinal Artery Occlusion.Semin Ophthalmol. 2024 Feb;39(2):129-138. doi: 10.1080/08820538.2023.2249539. Epub 2023 Aug 29. Semin Ophthalmol. 2024. PMID: 37644706 Review.
-
Acute central retinal artery occlusion treated with intravenous recombinant tissue plasminogen activator.J Stroke Cerebrovasc Dis. 2012 Nov;21(8):913.e5-8. doi: 10.1016/j.jstrokecerebrovasdis.2012.01.003. Epub 2012 Feb 18. J Stroke Cerebrovasc Dis. 2012. PMID: 22349707 Review.
Cited by
-
Macular vessel density in central retinal artery occlusion with retinal arterial cannulation.Sci Rep. 2023 Nov 8;13(1):19369. doi: 10.1038/s41598-023-46267-w. Sci Rep. 2023. PMID: 37938610 Free PMC article.
-
Update on central retinal artery occlusion.Indian J Ophthalmol. 2024 Jul 1;72(7):945-955. doi: 10.4103/IJO.IJO_2826_23. Epub 2024 Jun 22. Indian J Ophthalmol. 2024. PMID: 38905460 Free PMC article. Review.
-
Management of vision loss associated with complications of cosmetic filler injections.Front Ophthalmol (Lausanne). 2025 Apr 11;5:1568370. doi: 10.3389/fopht.2025.1568370. eCollection 2025. Front Ophthalmol (Lausanne). 2025. PMID: 40291837 Free PMC article. Review.
-
Intraoperative Cycling Pressure Variation in the Treatment of Central Retinal Artery Occlusion.Case Rep Ophthalmol Med. 2021 Jan 13;2021:6649657. doi: 10.1155/2021/6649657. eCollection 2021. Case Rep Ophthalmol Med. 2021. PMID: 33510922 Free PMC article.
-
Physical Enhancement? Nanocarrier? Current Progress in Transdermal Drug Delivery.Nanomaterials (Basel). 2021 Jan 28;11(2):335. doi: 10.3390/nano11020335. Nanomaterials (Basel). 2021. PMID: 33525364 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
