

Fluid balance concepts in medicine: Principles and practice
- PMID: 29359117
- PMCID: PMC5760509
- DOI: 10.5527/wjn.v7.i1.1
Fluid balance concepts in medicine: Principles and practice
Abstract
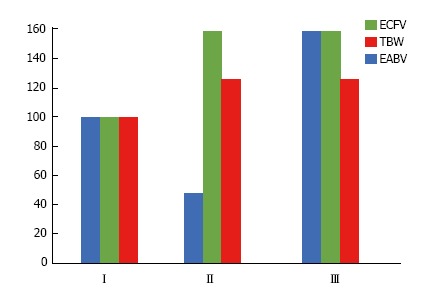
The regulation of body fluid balance is a key concern in health and disease and comprises three concepts. The first concept pertains to the relationship between total body water (TBW) and total effective solute and is expressed in terms of the tonicity of the body fluids. Disturbances in tonicity are the main factor responsible for changes in cell volume, which can critically affect brain cell function and survival. Solutes distributed almost exclusively in the extracellular compartment (mainly sodium salts) and in the intracellular compartment (mainly potassium salts) contribute to tonicity, while solutes distributed in TBW have no effect on tonicity. The second body fluid balance concept relates to the regulation and measurement of abnormalities of sodium salt balance and extracellular volume. Estimation of extracellular volume is more complex and error prone than measurement of TBW. A key function of extracellular volume, which is defined as the effective arterial blood volume (EABV), is to ensure adequate perfusion of cells and organs. Other factors, including cardiac output, total and regional capacity of both arteries and veins, Starling forces in the capillaries, and gravity also affect the EABV. Collectively, these factors interact closely with extracellular volume and some of them undergo substantial changes in certain acute and chronic severe illnesses. Their changes result not only in extracellular volume expansion, but in the need for a larger extracellular volume compared with that of healthy individuals. Assessing extracellular volume in severe illness is challenging because the estimates of this volume by commonly used methods are prone to large errors in many illnesses. In addition, the optimal extracellular volume may vary from illness to illness, is only partially based on volume measurements by traditional methods, and has not been determined for each illness. Further research is needed to determine optimal extracellular volume levels in several illnesses. For these reasons, extracellular volume in severe illness merits a separate third concept of body fluid balance.
Keywords: Body fluids; Body water; Congestive heart failure; Extracellular volume; Hepatic cirrhosis; Hypertonicity; Hypotonicity; Nephrotic syndrome; Sepsis.
Conflict of interest statement
Conflict-of-interest statement: Dominic SC Raj is supported by RO1 DK073665-01A1, 1U01DK099914-01 and IU01DK09924-01 from the National Institutes of Health. Joseph I Shapiro is supported by HL105649, HL071556 and HL109015 from the National Institutes of Health. The other authors declare no conflicts of interest.
Figures
References
-
- Wong LL, Verbalis JG. Systemic diseases associated with disorders of water homeostasis. Endocrinol Metab Clin North Am. 2002;31:121–140. - PubMed
-
- Adler SM, Verbalis JG. Disorders of body water homeostasis in critical illness. Endocrinol Metab Clin North Am. 2006;35:873–894, xi. - PubMed
-
- Hew-Butler T, Rosner MH, Fowkes-Godek S, Dugas JP, Hoffman MD, Lewis DP, Maughan RJ, Miller KC, Montain SJ, Rehrer NJ, et al. Statement of the 3rd International Exercise-Associated Hyponatremia Consensus Development Conference, Carlsbad, California, 2015. Br J Sports Med. 2015;49:1432–1446. - PubMed
-
- Manz F, Wentz A. The importance of good hydration for the prevention of chronic diseases. Nutr Rev. 2005;63:S2–S5. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
