

Prevalence, Presentation and Treatment of 'Balloon Undilatable' Chronic Total Occlusions: Insights from a Multicenter US Registry
- PMID: 29359452
- PMCID: PMC5849516
- DOI: 10.1002/ccd.27510
Prevalence, Presentation and Treatment of 'Balloon Undilatable' Chronic Total Occlusions: Insights from a Multicenter US Registry
Abstract
Background: The prevalence, treatment and outcomes of balloon undilatable chronic total occlusions (CTOs) have received limited study.
Methods: We examined the prevalence, clinical and angiographic characteristics, and procedural outcomes of percutaneous coronary interventions (PCIs) for balloon undilatable CTOs in a contemporary multicenter US registry.
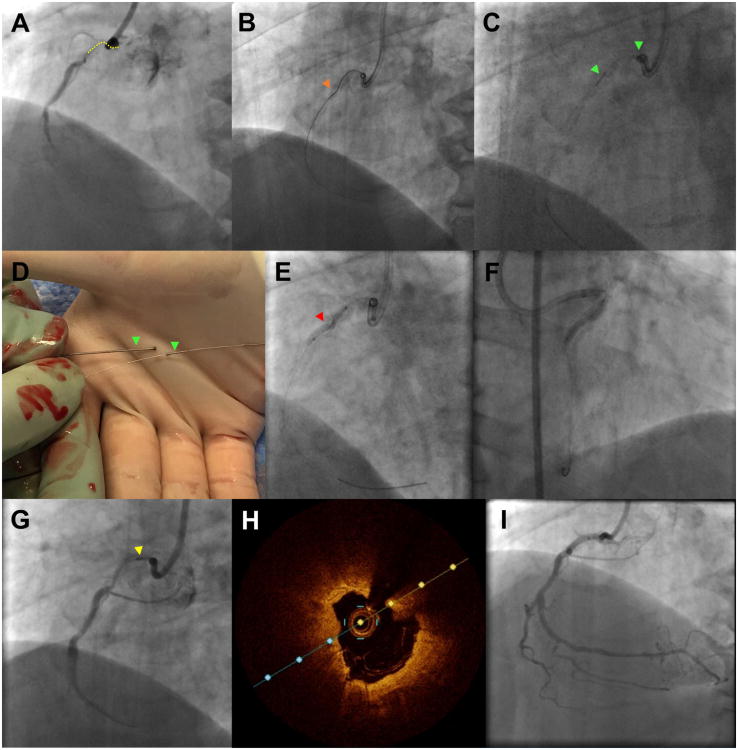
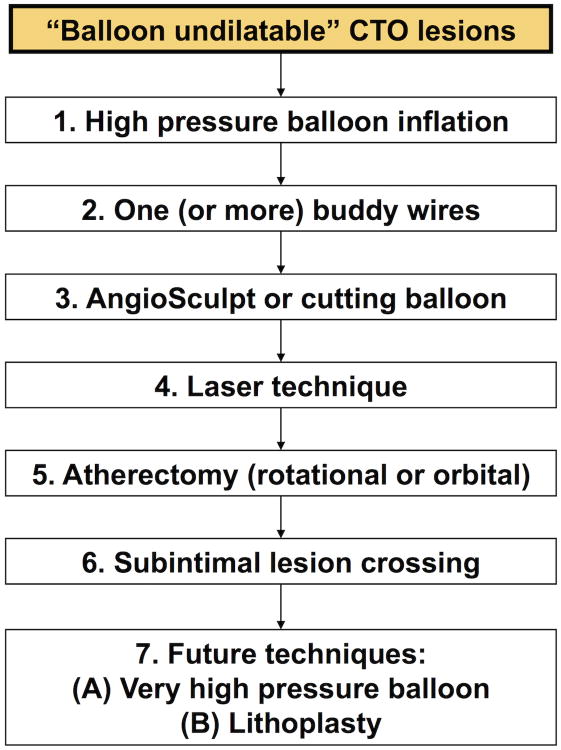
Results: Between 2012 and 2017 data on balloon undilatable lesions were available for 425 consecutive CTO PCIs in 415 patients in whom guidewire crossing was successful: 52 of 425 CTOs were balloon undilatable (12%). Mean patient age was 65 ± 10 years and most patients were men (84%). Patients with balloon undilatable CTOs were more likely to be diabetic (67 vs. 41%, P < 0.001) and have heart failure (44 vs. 28%, P = 0.027). Balloon undilatable CTOs were longer (40 mm [interquartile range, IQR 20-50] vs. 30 [IQR 15-40], P = 0.016), more likely to have moderate/severe calcification (87 vs. 54%, P < 0.001), and had higher J-CTO score (3.2 ± 1.1 vs. 2.5 ± 1.3, P < 0.001) and PROGRESS-CTO complications score (3.9 ± 1.7 vs. 3.1 ± 2.0, P < 0.005). They were associated with lower technical and procedural success (92 vs. 98%, P = 0.024; and 88 vs. 96%, P = 0.034, respectively) and higher risk for in-hospital major adverse events (8 vs. 2%, P = 0.008) due to higher perforation rates. The most frequent treatments for balloon undilatable CTOs were high pressure balloon inflations (64%), rotational atherectomy (31%), laser (21%), and cutting balloons (15%).
Conclusions: Balloon undilatable CTOs are common and are associated with lower success and higher complication rates.
Trial registration: ClinicalTrials.gov NCT02061436.
Keywords: chronic total occlusion; complex coronary intervention; percutaneous coronary intervention.
© 2018 Wiley Periodicals, Inc.
Figures
Comment in
-
Coronary chronic total occlusions: How to dilate the tough ones.Catheter Cardiovasc Interv. 2018 Mar 1;91(4):667-668. doi: 10.1002/ccd.27575. Catheter Cardiovasc Interv. 2018. PMID: 29532645
References
-
- Brilakis ES, Banerjee S, Karmpaliotis D, et al. Procedural Outcomes of Chronic Total Occlusion Percutaneous Coronary Intervention: A Report From the NCDR (National Cardiovascular Data Registry) JACC Cardiovasc Interv. 2015;8:245–53. - PubMed
-
- Galassi AR, Sianos G, Werner GS, et al. Retrograde Recanalization of Chronic Total Occlusions in Europe: Procedural, In-Hospital, and Long-Term Outcomes From the Multicenter ERCTO Registry. J Am Coll Cardiol. 2015;65:2388–400. - PubMed
-
- Wilson WM, Walsh SJ, Yan AT, et al. Hybrid approach improves success of chronic total occlusion angioplasty. Heart. 2016;102:1486–93. - PubMed
-
- Maeremans J, Walsh S, Knaapen P, et al. The Hybrid Algorithm for Treating Chronic Total Occlusions in Europe: The RECHARGE Registry. J Am Coll Cardiol. 2016;68:1958–1970. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
