

cHCC-CCA: Consensus terminology for primary liver carcinomas with both hepatocytic and cholangiocytic differentation
- PMID: 29360137
- PMCID: PMC6340292
- DOI: 10.1002/hep.29789
cHCC-CCA: Consensus terminology for primary liver carcinomas with both hepatocytic and cholangiocytic differentation
Abstract
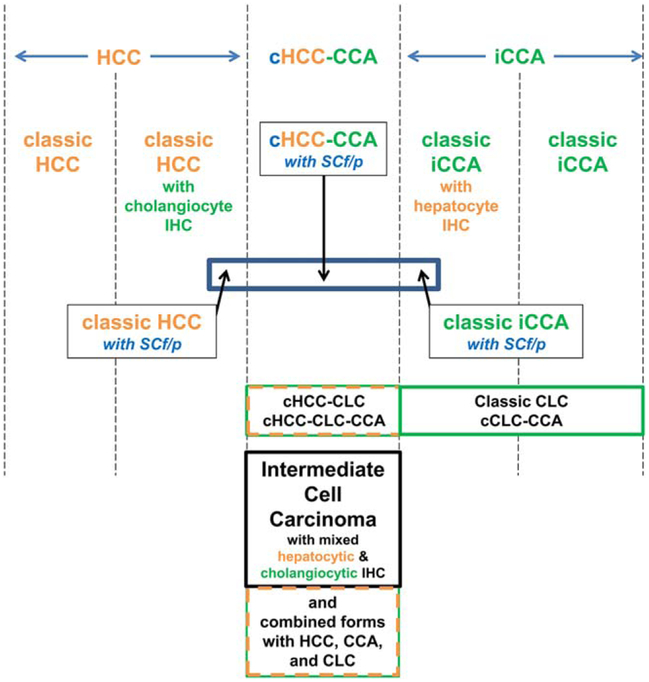
Primary liver carcinomas with both hepatocytic and cholangiocytic differentiation have been referred to as "combined (or mixed) hepatocellular-cholangiocarcinoma." These tumors, although described over 100 years ago, have attracted greater attention recently because of interest in possible stem cell origin and perhaps because of greater frequency and clinical recognition. Currently, because of a lack of common terminology in the literature, effective treatment and predictable outcome data have been challenging to accrue. This article represents a consensus document from an international community of pathologists, radiologists, and clinicians who have studied and reported on these tumors and recommends a working terminology for diagnostic and research approaches for further study and evaluation.
Conclusion: It is recommended that diagnosis is based on routine histopathology with hematoxylin and eosin (H&E); immunostains are supportive, but not essential for diagnosis. (Hepatology 2018;68:113-126).
© 2018 by the American Association for the Study of Liver Diseases.
Conflict of interest statement
Potential conflict of interest: Dr. Sirlin is on the speakers’ bureau for and received grants from GE. He is on the speakers’ bureau for Bayer. He received grants from Siemens. Dr. Kagen consults for and is on the speakers’ bureau for Bayer.
Figures
References
-
- Wells HG. Primary carcinoma of the liver. Am J M Sc 1903; 126:403–417.
-
- European Association for the Study of the Liver. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 2012;56:908–943. - PubMed
-
- Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of 100 cases among 48,900 necropsies. Cancer 1954;7:462–503. - PubMed
-
- Goodman ZD, Ishak KG, Langloss JM, Sesterhenn IA, Rabin L. Combined hepatocellular-cholangiocarcinoma. A histologic and immunohistochemical study. Cancer 1985;55:124–135. - PubMed
-
- Ng IO, Shek TW, Nicholls J, Ma LT. Combined hepatocellular-cholangiocarcinoma: a clinicopathological study. J Gastroenterol Hepatol 1998;13:34–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
