

Long-term risks and benefits associated with cesarean delivery for mother, baby, and subsequent pregnancies: Systematic review and meta-analysis
- PMID: 29360829
- PMCID: PMC5779640
- DOI: 10.1371/journal.pmed.1002494
Long-term risks and benefits associated with cesarean delivery for mother, baby, and subsequent pregnancies: Systematic review and meta-analysis
Abstract
Background: Cesarean birth rates continue to rise worldwide with recent (2016) reported rates of 24.5% in Western Europe, 32% in North America, and 41% in South America. The objective of this systematic review is to describe the long-term risks and benefits of cesarean delivery for mother, baby, and subsequent pregnancies. The primary maternal outcome was pelvic floor dysfunction, the primary baby outcome was asthma, and the primary subsequent pregnancy outcome was perinatal death.
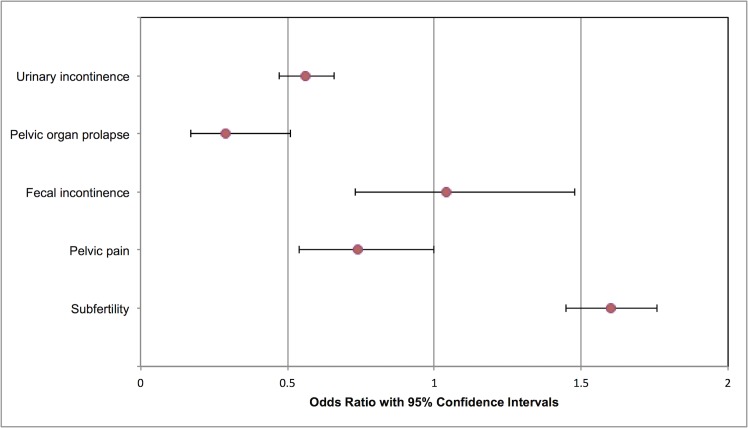
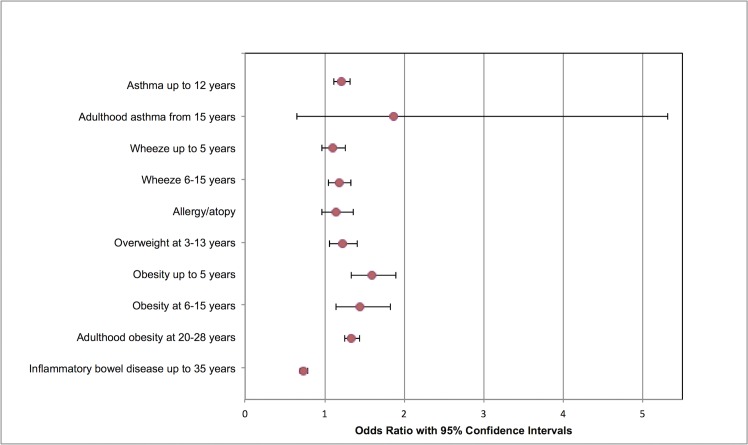
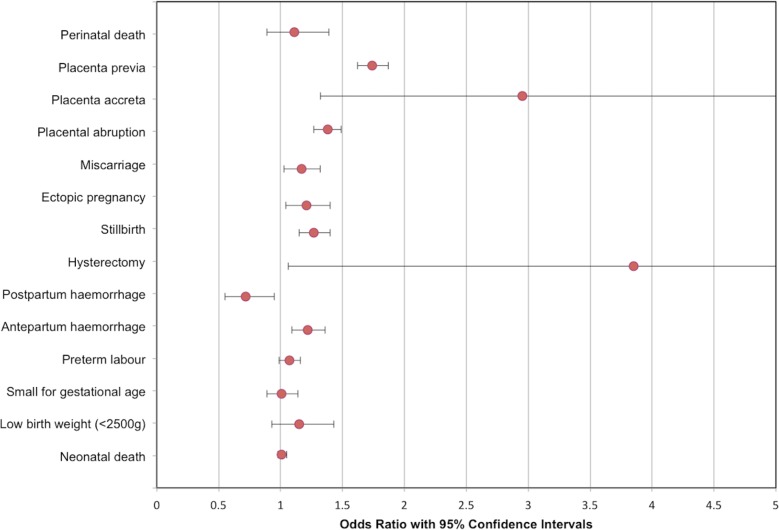
Methods and findings: Medline, Embase, Cochrane, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases were systematically searched for published studies in human subjects (last search 25 May 2017), supplemented by manual searches. Included studies were randomized controlled trials (RCTs) and large (more than 1,000 participants) prospective cohort studies with greater than or equal to one-year follow-up comparing outcomes of women delivering by cesarean delivery and by vaginal delivery. Two assessors screened 30,327 abstracts. Studies were graded for risk of bias by two assessors using the Scottish Intercollegiate Guideline Network (SIGN) Methodology Checklist and the Risk of Bias Assessment tool for Non-Randomized Studies. Results were pooled in fixed effects meta-analyses or in random effects models when significant heterogeneity was present (I2 ≥ 40%). One RCT and 79 cohort studies (all from high income countries) were included, involving 29,928,274 participants. Compared to vaginal delivery, cesarean delivery was associated with decreased risk of urinary incontinence, odds ratio (OR) 0.56 (95% CI 0.47 to 0.66; n = 58,900; 8 studies) and pelvic organ prolapse (OR 0.29, 0.17 to 0.51; n = 39,208; 2 studies). Children delivered by cesarean delivery had increased risk of asthma up to the age of 12 years (OR 1.21, 1.11 to 1.32; n = 887,960; 13 studies) and obesity up to the age of 5 years (OR 1.59, 1.33 to 1.90; n = 64,113; 6 studies). Pregnancy after cesarean delivery was associated with increased risk of miscarriage (OR 1.17, 1.03 to 1.32; n = 151,412; 4 studies) and stillbirth (OR 1.27, 1.15 to 1.40; n = 703,562; 8 studies), but not perinatal mortality (OR 1.11, 0.89 to 1.39; n = 91,429; 2 studies). Pregnancy following cesarean delivery was associated with increased risk of placenta previa (OR 1.74, 1.62 to 1.87; n = 7,101,692; 10 studies), placenta accreta (OR 2.95, 1.32 to 6.60; n = 705,108; 3 studies), and placental abruption (OR 1.38, 1.27 to 1.49; n = 5,667,160; 6 studies). This is a comprehensive review adhering to a registered protocol, and guidelines for the Meta-analysis of Observational Studies in Epidemiology were followed, but it is based on predominantly observational data, and in some meta-analyses, between-study heterogeneity is high; therefore, causation cannot be inferred and the results should be interpreted with caution.
Conclusions: When compared with vaginal delivery, cesarean delivery is associated with a reduced rate of urinary incontinence and pelvic organ prolapse, but this should be weighed against the association with increased risks for fertility, future pregnancy, and long-term childhood outcomes. This information could be valuable in counselling women on mode of delivery.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Betran AP, Ye J, Moller AB, Zhang J, Gulmezoglu AM, Torloni MR. The increasing trend in caesarean section rates: Global, regional and national estimates: 1990–2014. PLoS ONE. 2016;11(2):e0148343 doi: 10.1371/journal.pone.0148343 - DOI - PMC - PubMed
-
- Gibbons L, Belizan JM, Lauer JA, Betra AP, Merialdi M, Althabe F. The Global Numbers and Costs of Additionally Needed and Unnecessary Caesarean Sections Performed per Year: Overuse as a Barrier to Universal Coverage. World Health Report (2010). Background Paper, 30.
-
- Thomas J, Paranjothy S. Royal College of Obstetricians and Gynaecologists Clinical Effectiveness Support Unit. National Sentinel Caesarean Section Audit Report. RCOG Press; 2001.
-
- National Institute for Health and Clinical Excellence (2011) Caesarean Section (NICE Clinical Guideline 132). Available at: https://www.nice.org.uk/guidance/CG132 [Accessed 8th January 2018]. - PubMed
-
- Hannah ME, Whyte H, Hannah WJ, Hewson S, Amankwah K, Cheng M, et al. Maternal outcomes at 2 years after planned cesarean section versus planned vaginal birth for breech presentation at term: The international randomized Term Breech Trial. Am J Obstet Gynecol. 2004;191(3):917–27. doi: 10.1016/j.ajog.2004.08.004 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
