

Robot-assisted laparoscopic surgery versus conventional laparoscopic surgery in randomized controlled trials: A systematic review and meta-analysis
- PMID: 29360840
- PMCID: PMC5779699
- DOI: 10.1371/journal.pone.0191628
Robot-assisted laparoscopic surgery versus conventional laparoscopic surgery in randomized controlled trials: A systematic review and meta-analysis
Abstract
Importance: This review provides a comprehensive comparison of treatment outcomes between robot-assisted laparoscopic surgery (RLS) and conventional laparoscopic surgery (CLS) based on randomly-controlled trials (RCTs).
Objectives: We employed RCTs to provide a systematic review that will enable the relevant community to weigh the effectiveness and efficacy of surgical robotics in controversial fields on surgical procedures both overall and on each individual surgical procedure.
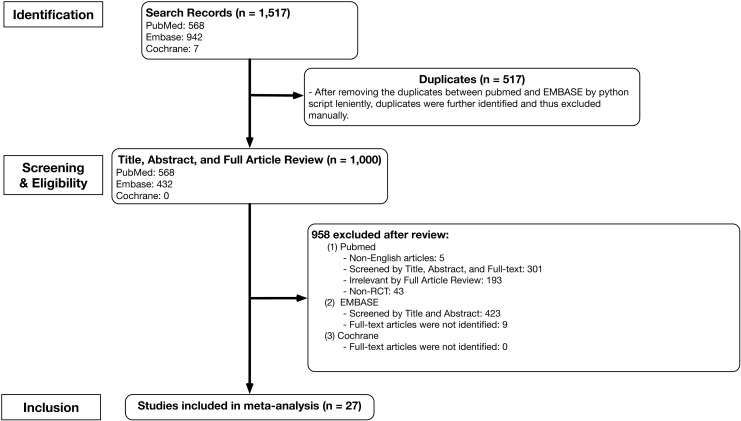
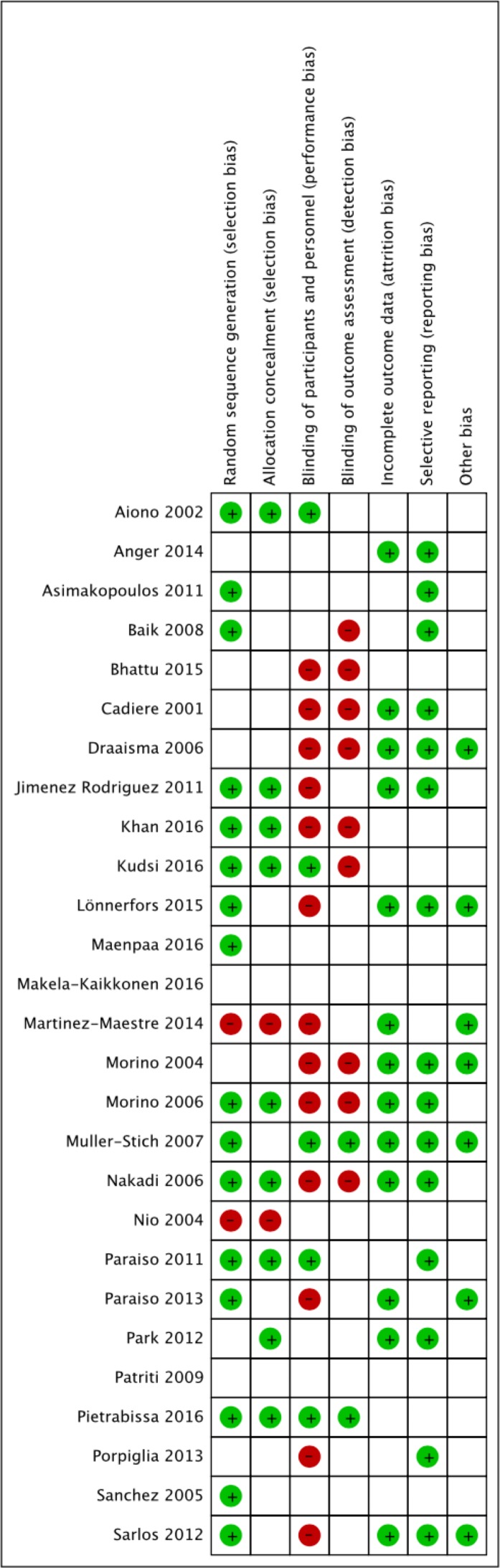
Evidence review: A search was conducted for RCTs in PubMed, EMBASE, and Cochrane databases from 1981 to 2016. Among a total of 1,517 articles, 27 clinical reports with a mean sample size of 65 patients per report (32.7 patients who underwent RLS and 32.5 who underwent CLS), met the inclusion criteria.
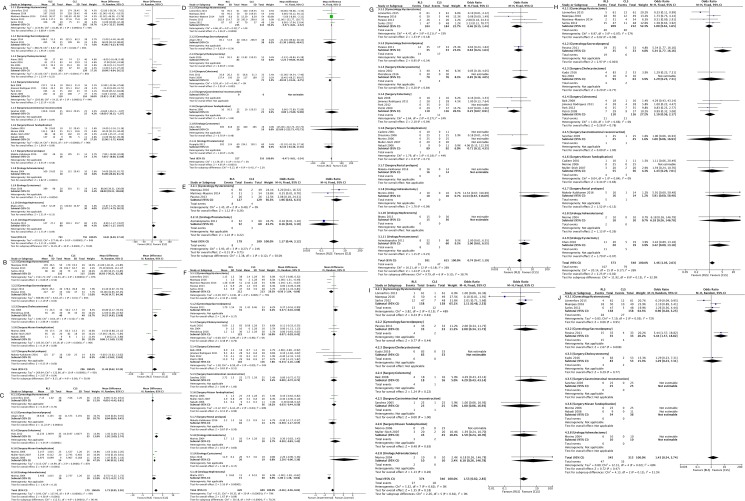
Findings: CLS shows significant advantages in total operative time, net operative time, total complication rate, and operative cost (p < 0.05 in all cases), whereas the estimated blood loss was less in RLS (p < 0.05). As subgroup analyses, conversion rate on colectomy and length of hospital stay on hysterectomy statistically favors RLS (p < 0.05).
Conclusions: Despite higher operative cost, RLS does not result in statistically better treatment outcomes, with the exception of lower estimated blood loss. Operative time and total complication rate are significantly more favorable with CLS.
Conflict of interest statement
Figures
References
-
- Liao G, Zhao Z, Lin S, Li R, Yuan Y, Du S, et al. Robotic-assisted versus laparoscopic colorectal surgery: a meta-analysis of four randomized controlled trials. World J Surg Oncol. 2014;12: 122 doi: 10.1186/1477-7819-12-122 - DOI - PMC - PubMed
-
- Tekkis PP, Senagore AJ, Delaney CP, Fazio VW. Evaluation of the learning curve in laparoscopic colorectal surgery: comparison of right-sided and left-sided resections. Ann Surg. 2005;242: 83–91. doi: 10.1097/01.sla.0000167857.14690.68 - DOI - PMC - PubMed
-
- Lin S, Jiang HG, Chen ZH, Zhou SY, Liu XS, Yu JR. Meta-analysis of robotic and laparoscopic surgery for treatment of rectal cancer. World J Gastroenterol. 2011;17: 5214–20. doi: 10.3748/wjg.v17.i47.5214 - DOI - PMC - PubMed
-
- O'Neill M, Moran PS, Teljeur C, O'Sullivan OE, O'Reilly BA, Hewitt M, et al. Robot-assisted hysterectomy compared to open and laparoscopic approaches: systematic review and meta-analysis. Arch Gynecol Obstet. 2013;287: 907–18. doi: 10.1007/s00404-012-2681-z - DOI - PubMed
-
- Brandao LF, Autorino R, Laydner H, Haber GP, Ouzaid I, De Sio M, et al. Robotic versus laparoscopic adrenalectomy: a systematic review and meta-analysis. Eur Urol. 2014;65: 1154–61. doi: 10.1016/j.eururo.2013.09.021 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
