

Attributable Healthcare Resource Utilization and Costs for Patients With Primary and Recurrent Clostridium difficile Infection in the United States
- PMID: 29360950
- PMCID: PMC5905590
- DOI: 10.1093/cid/cix1021
Attributable Healthcare Resource Utilization and Costs for Patients With Primary and Recurrent Clostridium difficile Infection in the United States
Abstract
Background: The economic burden of Clostridium difficile infection (CDI), the leading cause of nosocomial infectious diarrhea, is not well understood. The objective of this study was to estimate the healthcare resource utilization (HCRU) and costs attributable to primary CDI and recurrent CDI (rCDI).
Methods: This is a database (MarketScan) study. Patients without CDI were matched 1:1 by propensity score to those with primary CDI but no recurrences to obtain HCRU and costs attributable to primary CDI. Patients with primary CDI but no recurrences were matched 1:1 by propensity score to those with primary CDI plus 1 recurrence in order to obtain HCRU and costs attributable to rCDI. Adjusted estimates for incremental cumulative hospitalized days and healthcare costs over a 6-month follow-up period were obtained by generalized linear models with a Poisson or gamma distribution and a log link. Bootstrapping was used to obtain 95% confidence intervals (CIs).
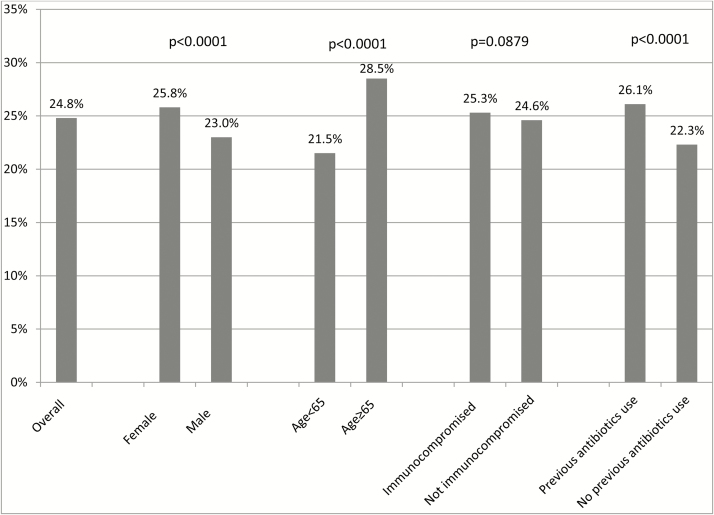
Results: A total of 55504 eligible CDI patients were identified. Approximately 25% of these CDI patients had rCDI. The cumulative hospitalized days attributable to primary CDI and rCDI over the 6-month follow-up period were 5.20 days (95% CI, 5.01-5.39) and 1.95 days (95% CI, 1.48-2.43), respectively. The healthcare costs attributable to primary CDI and rCDI over the 6-month follow-up period were $24205 (95% CI, $23436-$25013) and $10580 (95% CI, $8849-$12446), respectively.
Conclusions: The HCRU and costs attributable to primary CDI and rCDI are quite substantial. It is necessary to reduce the burden of CDI, especially rCDI.
Figures
References
-
- Kelly CP, LaMont JT. Clostridium difficile—more difficult than ever. N Engl J Med 2008; 359:1932–40. - PubMed
-
- Bignardi GE. Risk factors for Clostridium difficile infection. J Hosp Infect 1998; 40:1–15. - PubMed
-
- Johnson S. Recurrent Clostridium difficile infection: a review of risk factors, treatments, and outcomes. J Infect 2009; 58:403–10. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
