

Totally thoracoscopic ablation for atrial fibrillation: a systematic safety analysis
- PMID: 29361045
- PMCID: PMC6212776
- DOI: 10.1093/europace/eux385
Totally thoracoscopic ablation for atrial fibrillation: a systematic safety analysis
Abstract
Aims: Thoracoscopic surgical ablation has evolved into a successful strategy for symptomatic atrial fibrillation (AF) refractory to other therapy. More widespread referral is limited by the lack of information on potential complications. Our aim was to systematically evaluate 30-day complications of totally thoracoscopic surgical ablation.
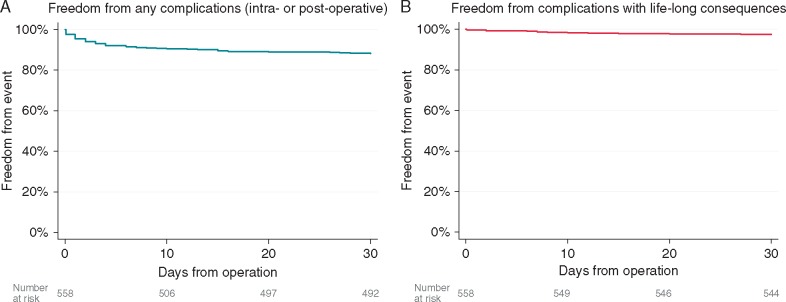
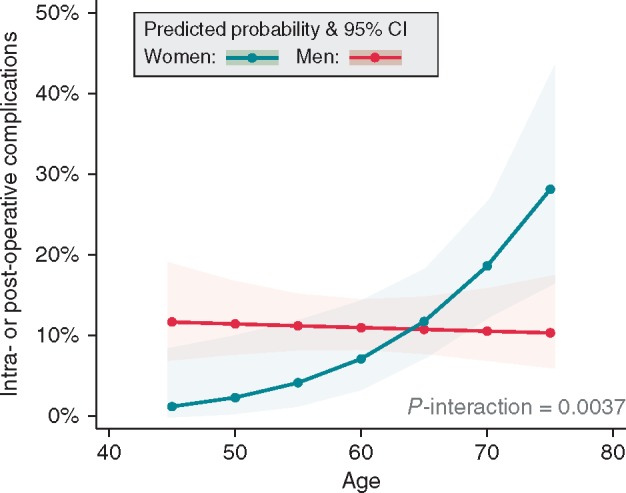
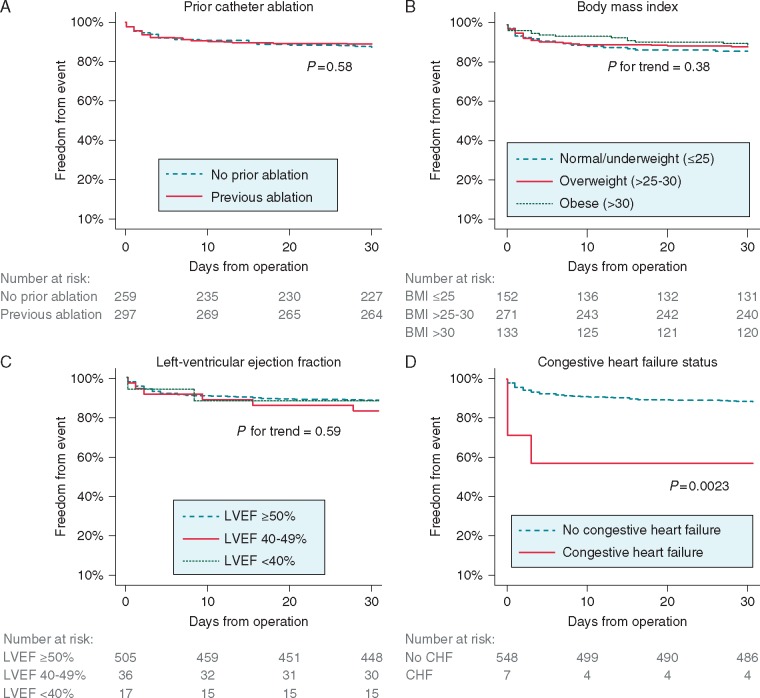
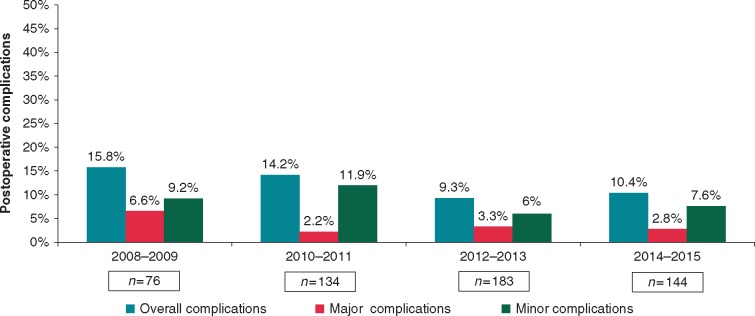
Methods and results: We retrospectively studied consecutive patients undergoing totally thoracoscopic surgical ablation at a referral centre in the Netherlands (2007-2016). Patients received pulmonary vein isolation, with additional lesion lines as needed, and left atrial appendage exclusion. The primary outcomes were freedom from any complications and freedom from irreversible complications at 30-days. Secondary outcomes included intra- and post-operative complications according to severity. Included were 558 patients with median age 62 years (interquartile range 56-68 years), 70% male and 53% with a previous failed catheter ablation. The cohort consisted of 43% paroxysmal AF, 47% persistent AF, and 10% long-standing persistent AF. Freedom from any 30-day complication was 88.2%, and from complications with life-long affecting consequences 97.5%. The intra-operative complication rate was 2.3% with no strokes or death observed. The median hospital length of stay was 4 days. The percentage of patients with major and minor complications at 30-days was 3.2% and 8.1%, respectively, with one patient dying of an ischaemic stroke. The only patient groups with excess complications were women aged ≥70 years and patients with a history of congestive heart failure.
Conclusions: Totally thoracoscopic ablation is associated with a low complication rate in a referral centre and may be a useful alternative to other rhythm control strategies.
Figures
References
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B. et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace 2016;18:1609–78. - PubMed
-
- Boersma LV, Castella M, van Boven W, Berruezo A, Yilmaz A, Nadal M. et al. Atrial fibrillation catheter ablation versus surgical ablation treatment (FAST): a 2-center randomized clinical trial. Circulation 2012;125:23–30. - PubMed
-
- Van Laar C, Kelder J, van Putte BP.. The totally thoracoscopic maze procedure for the treatment of atrial fibrillation. Interact Cardiovasc Thorac Surg 2017;24:102–11. - PubMed
-
- Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA. et al. 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace 2012;14:528–606. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
