

Patients with melanoma treated with an anti-PD-1 antibody beyond RECIST progression: a US Food and Drug Administration pooled analysis
- PMID: 29361469
- PMCID: PMC5806609
- DOI: 10.1016/S1470-2045(17)30846-X
Patients with melanoma treated with an anti-PD-1 antibody beyond RECIST progression: a US Food and Drug Administration pooled analysis
Abstract
Background: Patients who receive immunotherapeutic drugs might develop an atypical response pattern, wherein they initially meet conventional response criteria for progressive disease but later have decreases in tumour burden. Such responses warrant further investigation into the potential benefits and risks for patients who continue immunotherapy beyond disease progression defined by the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1.
Methods: For this pooled analysis, we included all submissions of trial reports and data to the US Food and Drug Administration (FDA) in support of marketing applications for anti-programmed death receptor-1 (PD-1) antibodies (alone or in combination) for the treatment of patients with unresectable or metastatic melanoma that allowed for continuation of the antibody beyond RECIST-defined progression in the anti-PD-1 group and were approved by FDA before Jan 1, 2017. To investigate the effect of treatment beyond progression in patients with metastatic melanoma and to better characterise which of these patients would benefit from extended treatment, we pooled individual patient data from patients who received at least one dose of an anti-PD-1 antibody in the included trials. We included any patient receiving the anti-PD-1 antibody after their RECIST-defined progression date in the treatment beyond progression cohort and analysed them descriptively at baseline and at time of progression versus the cohort not receiving treatment beyond progression. We analysed the target lesion response after progression in patients in the treatment beyond progression cohort relative to progressive disease and baseline target lesion burden. We defined a treatment beyond progression response as a decrease in target lesion tumour burden (sum of the reference diameters) of at least 30% from the burden at the time of RECIST-defined progression that did not require confirmation at a subsequent assessment. We also compared individual timepoint responses, overall survival, and adverse events in the treatment beyond progression versus no treatment beyond progression cohorts.
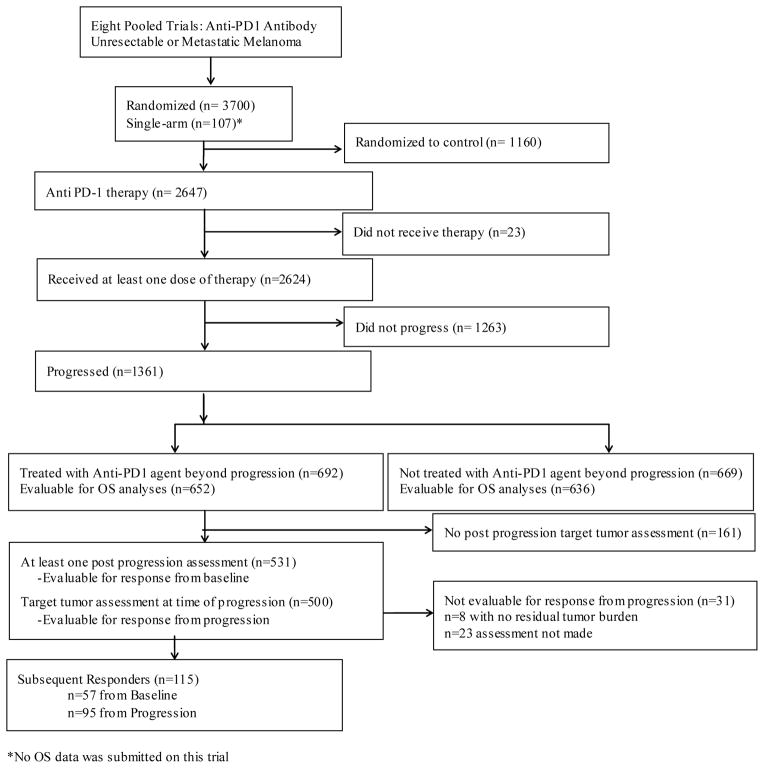
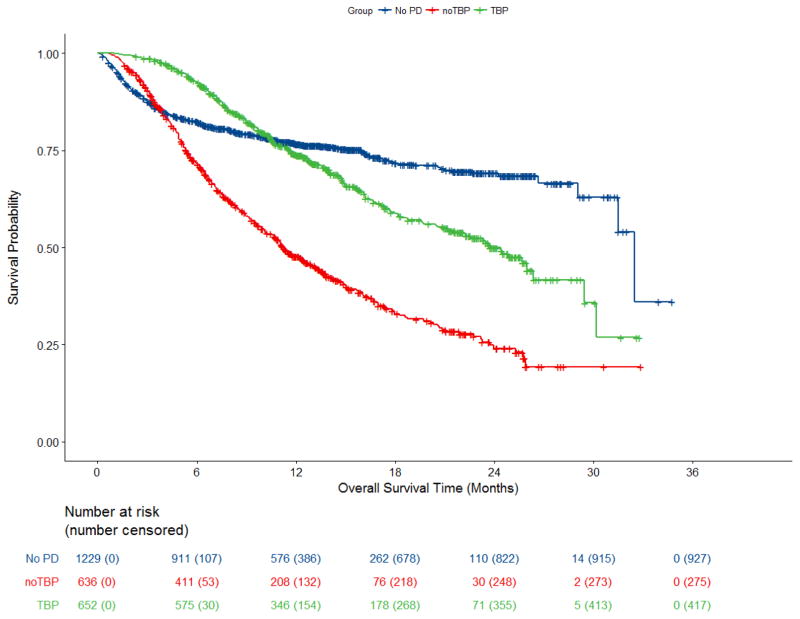
Findings: Among the eight multicentre clinical trials meeting this study's inclusion criteria, we pooled the data from 2624 patients receiving immunotherapy. 1361 (52%) had progressive disease, of whom 692 (51%) received continued anti-PD-1 antibody treatment beyond RECIST-defined progression and 669 (49%) did not. 95 (19%) of 500 patients in the treatment beyond progresssion cohort with evaluable assessments had a 30% or more decrease in tumour burden, when considering burden at RECIST-defined progression as the reference point, representing 14% of the 692 patients treated beyond progression and 4% of all 2624 patients treated with immunotherapy. Median overall survival in patients with RECIST-defined progressive disease given anti-PD-1 antibody was longer in the treatment beyond progression cohort (24·4 months, 95% CI 21·2-26·3) than in the cohort of patients who did not receive treatment beyond progression (11·2 months, 10·1-12·9). 362 (54%) of 669 patients in the no treatment beyond progression cohort had a serious adverse event up to 90 days after treatment discontinuation compared with 295 (43%) of 692 patients in the treatment beyond progression cohort. Immune-related adverse events that occurred up to 90 days from discontinuation were similar between the treatment beyond progression cohort (78 [11%] of 692 patients) and the no treatment beyond progression cohort (106 [16%] of 669).
Interpretation: Continuation of treatment beyond progression in the product labelling of these immunotherapies has not been recommended because the clinical benefit remains to be proven. Treatment beyond progression with anti-PD-1 antibody therapy might be appropriate for selected patients with unresectable or metastatic melanoma, identified by specific criteria at the time of progression, based on the potential for late responses in the setting of the known toxicity profile.
Funding: None.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
JC worked on this research while an FDA employee, and no longer contributed after leaving the agency; at the time of manuscript submission, JC is an employee of AstraZeneca. No potential conflicts of interest were disclosed by the remaining authors.
Figures
Comment in
-
Revisiting RECIST: the case of treatment beyond progression.Lancet Oncol. 2018 Feb;19(2):157-159. doi: 10.1016/S1470-2045(18)30007-X. Epub 2018 Jan 18. Lancet Oncol. 2018. PMID: 29361472 No abstract available.
-
Anti-PD-1 antibody treatment for melanoma.Lancet Oncol. 2018 May;19(5):e219. doi: 10.1016/S1470-2045(18)30202-X. Lancet Oncol. 2018. PMID: 29726378 No abstract available.
-
Anti-PD-1 antibody treatment for melanoma - Authors' reply.Lancet Oncol. 2018 May;19(5):e220. doi: 10.1016/S1470-2045(18)30251-1. Lancet Oncol. 2018. PMID: 29726379 No abstract available.
References
-
- Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1. 1) Eur J Cancer. 2009;45(2):228–47. - PubMed
-
- Wolchok JD, Hoos A, O’Day S, et al. Guidelines for the evaluation of immune therapy activity in solid tumors: immune-related response criteria. Clin Cancer Res. 2009;15(23):7412–20. - PubMed
-
- O’Day SJ, Maio M, Chiarion-Sileni V, et al. Efficacy and safety of ipilimumab monotherapy in patients with pretreated advanced melanoma: a multicenter single-arm phase II study. Ann Oncol. 21(8):1712–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
