

Prexasertib, a cell cycle checkpoint kinase 1 and 2 inhibitor, in BRCA wild-type recurrent high-grade serous ovarian cancer: a first-in-class proof-of-concept phase 2 study
- PMID: 29361470
- PMCID: PMC7366122
- DOI: 10.1016/S1470-2045(18)30009-3
Prexasertib, a cell cycle checkpoint kinase 1 and 2 inhibitor, in BRCA wild-type recurrent high-grade serous ovarian cancer: a first-in-class proof-of-concept phase 2 study
Abstract
Background: High-grade serous ovarian carcinoma is characterised by TP53 mutations, DNA repair defects, and genomic instability. We hypothesised that prexasertib (LY2606368), a cell cycle checkpoint kinase 1 and 2 inhibitor, would be active in BRCA wild-type disease.
Methods: In an open-label, single-centre, two-stage, proof-of-concept phase 2 study, we enrolled women aged 18 years or older with measurable, recurrent high-grade serous or high-grade endometrioid ovarian carcinoma. All patients had a negative family history of hereditary breast and ovarian cancer or known BRCA wild-type status, measurable disease according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1, Eastern Cooperative Oncology Group performance status score 0-2, and adequate haematological, renal, hepatic, and bone-marrow function. Patients received intravenous prexasertib 105 mg/m2 administered over 1 h every 14 days in 28-day cycles until disease progression, unacceptable toxicity, or withdrawal of consent. The primary endpoint of investigator-assessed tumour response, based on RECIST version 1.1, was assessed per protocol (assessable patients who had undergone CT imaging at baseline and attended at least one protocol-specified follow-up) and by intention to treat. The final analysis of this cohort of patients with BRCA wild-type high-grade serous ovarian carcinoma is reported here. This ongoing trial is registered with ClinicalTrials.gov, number NCT02203513, and continues to enrol patients for the BRCA-mutated ovarian cancer cohort.
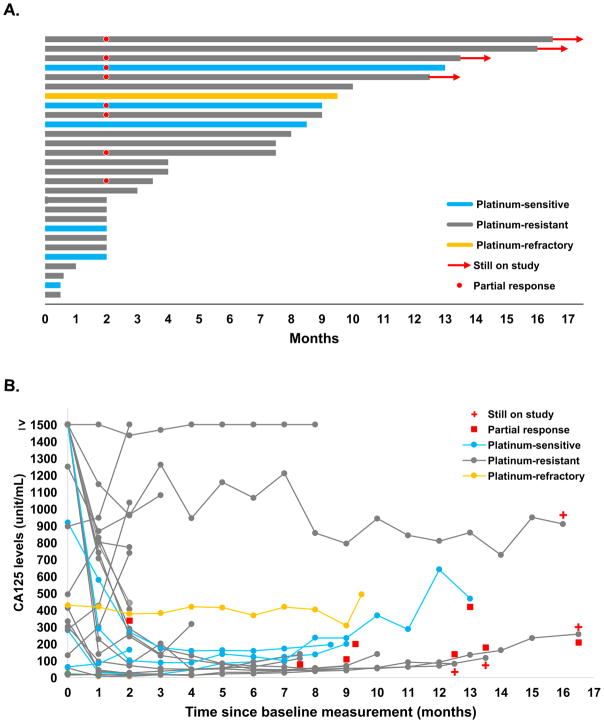
Findings: Between Jan 20, 2015, and Nov 2, 2016, we enrolled 28 women with a median age of 64 years (IQR 58·0-69·5) who had previously received a median of 5·0 (IQR 2·5-5·0) systemic therapies. Most patients (22 [79%]) had platinum-resistant or platinum-refractory disease. All women received at least one dose of prexasertib, but four (14%) of 28 patients were not assessable for RECIST response. Eight (33%, 95% CI 16-55) of 24 patients assessable per protocol had partial responses. In the intention-to-treat population, eight (29%, 95% CI 13-49) of 28 had a partial responses. The most common (in >10% patients) grade 3 or 4 treatment-emergent adverse events were neutropenia in 26 (93%) of 28 patients, reduced white blood cell count in 23 (82%), thrombocytopenia in seven (25%), and anaemia in three (11%). Grade 4 neutropenia was reported in 22 (79%) patients after the first dose of prexasertib and was transient (median duration 6 days [IQR 4-8]) and recovered without growth-factor support in all cases. The treatment-related serious adverse event of grade 3 febrile neutropenia was reported in two (7%) patients. One patient died during the study due to tumour progression.
Interpretation: Prexasertib showed clinical activity and was tolerable in patients with BRCA wild-type high-grade serous ovarian carcinoma. This drug warrants further development in this setting, especially for patients with platinum-resistant or platinum-refractory disease.
Funding: Intramural Research Program of the National Institutes of Health and National Cancer Institute.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
All authors declared no conflicts of interest.
Figures


Comment in
-
A turning point in the fight against ovarian cancer?Lancet Oncol. 2018 Feb;19(2):154-156. doi: 10.1016/S1470-2045(18)30005-6. Epub 2018 Jan 18. Lancet Oncol. 2018. PMID: 29361471 No abstract available.
Similar articles
-
Rucaparib in relapsed, platinum-sensitive high-grade ovarian carcinoma (ARIEL2 Part 1): an international, multicentre, open-label, phase 2 trial.Lancet Oncol. 2017 Jan;18(1):75-87. doi: 10.1016/S1470-2045(16)30559-9. Epub 2016 Nov 29. Lancet Oncol. 2017. PMID: 27908594 Clinical Trial.
-
Olaparib combined with chemotherapy for recurrent platinum-sensitive ovarian cancer: a randomised phase 2 trial.Lancet Oncol. 2015 Jan;16(1):87-97. doi: 10.1016/S1470-2045(14)71135-0. Epub 2014 Dec 4. Lancet Oncol. 2015. PMID: 25481791 Clinical Trial.
-
Maintenance olaparib for patients with newly diagnosed advanced ovarian cancer and a BRCA mutation (SOLO1/GOG 3004): 5-year follow-up of a randomised, double-blind, placebo-controlled, phase 3 trial.Lancet Oncol. 2021 Dec;22(12):1721-1731. doi: 10.1016/S1470-2045(21)00531-3. Epub 2021 Oct 26. Lancet Oncol. 2021. PMID: 34715071 Clinical Trial.
-
Prexasertib: an investigational checkpoint kinase inhibitor for the treatment of high-grade serous ovarian cancer.Expert Opin Investig Drugs. 2020 Aug;29(8):779-792. doi: 10.1080/13543784.2020.1783238. Epub 2020 Jun 25. Expert Opin Investig Drugs. 2020. PMID: 32539469 Review.
-
Homologous Recombination Deficiency Testing to Inform Patient Decisions About Niraparib Maintenance Therapy for High-Grade Serous or Endometrioid Epithelial Ovarian Cancer: A Health Technology Assessment.Ont Health Technol Assess Ser. 2023 Aug 10;23(5):1-188. eCollection 2023. Ont Health Technol Assess Ser. 2023. PMID: 37637244 Free PMC article.
Cited by
-
Gynecologic Cancer InterGroup CA125 response has a high negative predictive value for CHK1 inhibitor RECIST response in recurrent ovarian cancer.Sci Rep. 2024 Jul 29;14(1):17459. doi: 10.1038/s41598-024-68338-2. Sci Rep. 2024. PMID: 39075200 Free PMC article.
-
CNS penetration and pharmacodynamics of the CHK1 inhibitor prexasertib in a mouse Group 3 medulloblastoma model.Eur J Pharm Sci. 2020 Jan 15;142:105106. doi: 10.1016/j.ejps.2019.105106. Epub 2019 Oct 25. Eur J Pharm Sci. 2020. PMID: 31669383 Free PMC article.
-
Compassion and Empathy in Basic Medical Science Teaching: A Suggested Model.Cureus. 2021 Dec 6;13(12):e20205. doi: 10.7759/cureus.20205. eCollection 2021 Dec. Cureus. 2021. PMID: 35004025 Free PMC article.
-
Cell cycle checkpoints and beyond: Exploiting the ATR/CHK1/WEE1 pathway for the treatment of PARP inhibitor-resistant cancer.Pharmacol Res. 2022 Apr;178:106162. doi: 10.1016/j.phrs.2022.106162. Epub 2022 Mar 5. Pharmacol Res. 2022. PMID: 35259479 Free PMC article. Review.
-
DNA Repair and Ovarian Carcinogenesis: Impact on Risk, Prognosis and Therapy Outcome.Cancers (Basel). 2020 Jun 28;12(7):1713. doi: 10.3390/cancers12071713. Cancers (Basel). 2020. PMID: 32605254 Free PMC article. Review.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA Cancer J Clin. 2017;67:7–30. - PubMed
-
- Naumann RW, Coleman RL. Management strategies for recurrent platinum-resistant ovarian cancer. Drugs. 2011;71:1397–412. - PubMed
-
- Lin AB, McNeely SC, Beckmann RP. Achieving Precision Death with Cell-Cycle Inhibitors that Target DNA Replication and Repair. Clin Cancer Res. 2017;23:3232–40. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
