

Treatment Strategy for Dyslipidemia in Cardiovascular Disease Prevention: Focus on Old and New Drugs
- PMID: 29361723
- PMCID: PMC5874549
- DOI: 10.3390/pharmacy6010010
Treatment Strategy for Dyslipidemia in Cardiovascular Disease Prevention: Focus on Old and New Drugs
Abstract
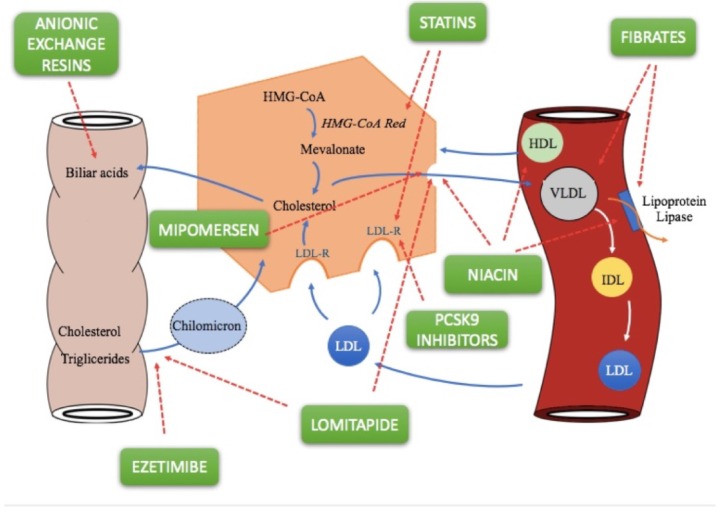
Prevention and treatment of dyslipidemia should be considered as an integral part of individual cardiovascular prevention interventions, which should be addressed primarily to those at higher risk who benefit most. To date, statins remain the first-choice therapy, as they have been shown to reduce the risk of major vascular events by lowering low-density lipoprotein cholesterol (LDL-C). However, due to adherence to statin therapy or statin resistance, many patients do not reach LDL-C target levels. Ezetimibe, fibrates, and nicotinic acid represent the second-choice drugs to be used in combination with statins if lipid targets cannot be reached. In addition, anti-PCSK9 drugs (evolocumab and alirocumab) provide an effective solution for patients with familial hypercholesterolemia (FH) and statin intolerance at very high cardiovascular risk. Recently, studies demonstrated the effects of two novel lipid-lowering agents (lomitapide and mipomersen) for the management of homozygous FH by decreasing LDL-C values and reducing cardiovascular events. However, the costs for these new therapies made the cost-effectiveness debate more complicated.
Keywords: PCSK9 inhibitors; dyslipidemia; fibrate; lipid lowering therapy; lomitapide; statins.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Management of Hypercholesterolemia, Appropriateness of Therapeutic Approaches and New Drugs in Patients with High Cardiovascular Risk.High Blood Press Cardiovasc Prev. 2016 Sep;23(3):217-30. doi: 10.1007/s40292-016-0155-2. Epub 2016 Aug 27. High Blood Press Cardiovasc Prev. 2016. PMID: 27567901 Free PMC article. Review.
-
2017 Taiwan lipid guidelines for high risk patients.J Formos Med Assoc. 2017 Apr;116(4):217-248. doi: 10.1016/j.jfma.2016.11.013. Epub 2017 Feb 24. J Formos Med Assoc. 2017. PMID: 28242176 Review.
-
New LDL-cholesterol lowering therapies: pharmacology, clinical trials, and relevance to acute coronary syndromes.Clin Ther. 2013 Aug;35(8):1082-98. doi: 10.1016/j.clinthera.2013.06.019. Epub 2013 Aug 8. Clin Ther. 2013. PMID: 23932550 Review.
-
Cost-effectiveness of PCSK9 Inhibitor Therapy in Patients With Heterozygous Familial Hypercholesterolemia or Atherosclerotic Cardiovascular Disease.JAMA. 2016 Aug 16;316(7):743-53. doi: 10.1001/jama.2016.11004. JAMA. 2016. PMID: 27533159
-
[The role of PCSK9-inhibitors and of lipoprotein apheresis in the treatment of homozygous and severe heterozygous familial hypercholesterolemia: A rivalry, or are things quite different?].Vnitr Lek. 2018 Winter;64(1):43-50. Vnitr Lek. 2018. PMID: 29498875 Czech.
Cited by
-
A comprehensive review on apolipoproteins as nontraditional cardiovascular risk factors in end-stage renal disease: current evidence and perspectives.Int Urol Nephrol. 2019 Jul;51(7):1173-1189. doi: 10.1007/s11255-019-02170-w. Epub 2019 May 22. Int Urol Nephrol. 2019. PMID: 31119518 Review.
-
LDL-cholesterol change and goal attainment following statin intensity titration among Asians in primary care: a retrospective cohort study.Lipids Health Dis. 2021 Jan 6;20(1):2. doi: 10.1186/s12944-020-01427-z. Lipids Health Dis. 2021. PMID: 33407522 Free PMC article.
-
Two Triterpenoids, ARM-2 and RA-5, From Protorhus longifolia Exhibit the Potential to Modulate Lipolysis and Lipogenesis in Cultured 3T3-L1 Adipocytes.J Lipids. 2024 Oct 17;2024:3972941. doi: 10.1155/2024/3972941. eCollection 2024. J Lipids. 2024. PMID: 39450349 Free PMC article.
-
The effects of rice bran supplementation for management of blood lipids: A GRADE-assessed systematic review, dose-response meta-analysis, and meta-regression of randomized controlled trials.Syst Rev. 2023 Apr 12;12(1):65. doi: 10.1186/s13643-023-02228-y. Syst Rev. 2023. PMID: 37046340 Free PMC article.
-
Stachys sieboldii Miq. Root Attenuates Weight Gain and Dyslipidemia in Rats on a High-Fat and High-Cholesterol Diet.Nutrients. 2020 Jul 11;12(7):2063. doi: 10.3390/nu12072063. Nutrients. 2020. PMID: 32664607 Free PMC article.
References
-
- Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults Treatment of high blood cholesterol in, executive summary of the third report of the national cholesterol Education program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment Panel III) JAMA. 2001;285:2486–2497. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
