

Shifting breast cancer surveillance from current hospital setting to a community based setting: a cost-effectiveness study
- PMID: 29361911
- PMCID: PMC5781302
- DOI: 10.1186/s12885-018-3992-7
Shifting breast cancer surveillance from current hospital setting to a community based setting: a cost-effectiveness study
Abstract
Background: This study explores the effectiveness and cost-effectiveness of surveillance after breast cancer treatment provided in a hospital-setting versus surveillance embedded in the community-based National Breast Cancer Screening Program (NBCSP).
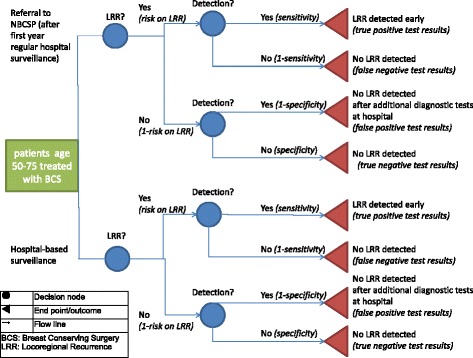
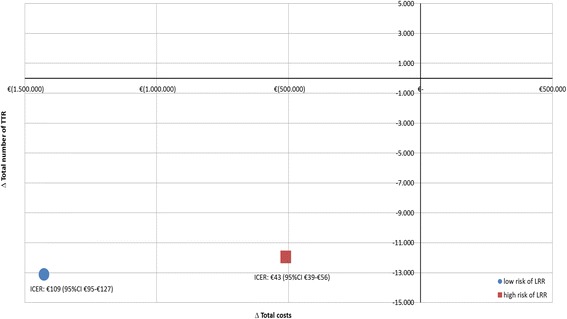
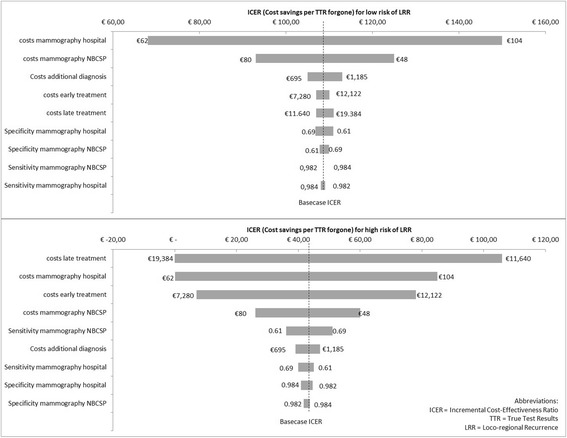
Methods: Using a decision tree, strategies were compared on effectiveness and costs from a healthcare perspective over a 5-year time horizon. Women aged 50-75 without distant metastases that underwent breast conserving surgery in 2003-2006 were selected from the Netherlands Cancer Registry (n = 14,093). Key input parameters were mammography sensitivity and specificity, risk of loco regional recurrence (LRR), and direct healthcare costs. Primary outcome measure was the proportion true test results (TTR), expressed as the positive and negative predictive value (PPV, NPV). The incremental cost-effectiveness ratio (ICER) is defined as incremental costs per TTR forgone.
Results: For the NBCSP-strategy, 13,534 TTR (8 positive; 13,526 negative), and 12,923 TTR (387 positive; 12,536 negative) were found for low and high risks respectively. For the hospital-based strategy, 26,663 TTR (13 positive; 26,650 negative) and 24,883 TTR (440 positive; 24,443 negative) were found for low and high risks respectively. For low risks, the PPV and NPV for the NBCSP-based strategy were 3.31% and 99.88%, and 2.74% and 99.95% for the hospital strategy respectively. For high risks, the PPV and NPV for the NBCSP-based strategy were 64.10% and 98.87%, and 50.98% and 99.71% for the hospital-based strategy respectively. Total expected costs of the NBCSP-based strategy were lower than for the hospital-based strategy (low risk: €1,271,666 NBCSP vs €2,698,302 hospital; high risk: €6,939,813 NBCSP vs €7,450,150 hospital), rendering ICERs that indicate cost savings of €109 (95%CI €95-€127) (low risk) and €43 (95%CI €39-€56) (high risk) per TTR forgone.
Conclusion: Despite expected cost-savings of over 50% in the NBCSP-based strategy, it is nearly 50% lower accurate than the hospital-based strategy, compromising the goal of early detection of LRR to an extent that is unlikely to be acceptable.
Keywords: Breast cancer; Cost-effectiveness; Loco regional recurrence; Screening; Surveillance.
Conflict of interest statement
Ethics approval and consent to participate
According to the Central Committee on Research involving Human Subjects (CCMO), this type of study does not require approval from an ethics committee in the Netherlands. This study was approved by the Privacy Review Board of the Netherlands Cancer Registry. All cancer patients are opted-in in the Netherlands Cancer Registry as defined by Dutch law, unless patients object to this. No formal consent is required.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Netherlands Comprehensive Cancer Organisation (IKNL). Dutch Cancer Figures n.d. http://www.cijfersoverkanker.nl/. Accessed 1 Jan 2016.
-
- Netherlands Comprehensive Cancer Organisation (IKNL). National guideline on breast cancer, version: 2.0. 2012.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
