

Cost-effectiveness of FreeO2 in patients with chronic obstructive pulmonary disease hospitalised for acute exacerbations: analysis of a pilot study in Quebec
- PMID: 29362258
- PMCID: PMC5786115
- DOI: 10.1136/bmjopen-2017-018835
Cost-effectiveness of FreeO2 in patients with chronic obstructive pulmonary disease hospitalised for acute exacerbations: analysis of a pilot study in Quebec
Abstract
Objective: Conduct a cost-effectiveness analysis of FreeO2 technology versus manual oxygen-titration technology for patients with chronic obstructive pulmonary disease (COPD) hospitalised for acute exacerbations.
Setting: Tertiary acute care hospital in Quebec, Canada.
Participants: 47 patients with COPD hospitalised for acute exacerbations.
Intervention: An automated oxygen-titration and oxygen-weaning technology.
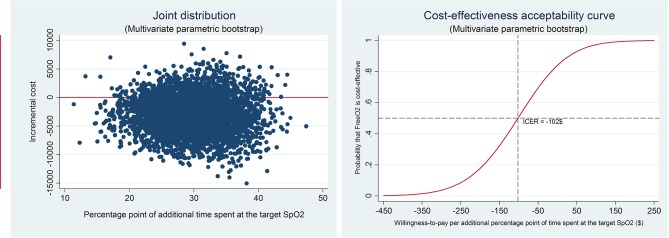
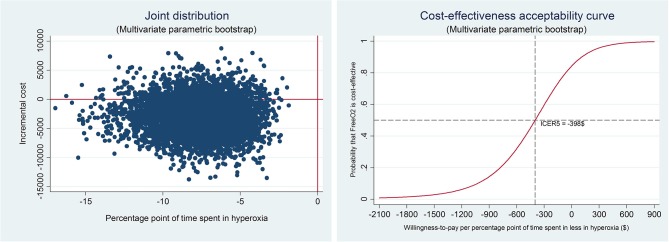
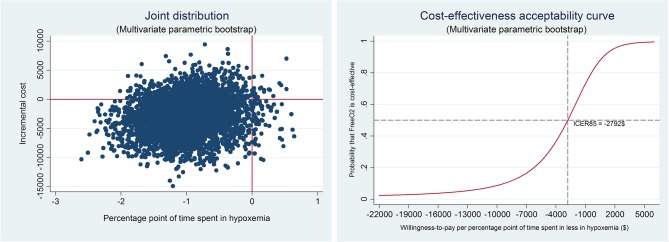
Methods and outcomes: The costs for hospitalisation and follow-up for 180 days were calculated using a microcosting approach and included the cost of FreeO2 technology. Incremental cost-effectiveness ratios (ICERs) were calculated using bootstrap resampling with 5000 replications. The main effect variable was the percentage of time spent at the target oxygen saturation (SpO2). The other two effect variables were the time spent in hyperoxia (target SpO2+5%) and in severe hypoxaemia (SpO2 <85%). The resamplings were based on data from a randomised controlled trial with 47 patients with COPD hospitalised for acute exacerbations.
Results: FreeO2 generated savings of 20.7% of the per-patient costs at 180 days (ie, -$C2959.71). This decrease is nevertheless not significant at the 95% threshold (P=0.13), but the effect variables all improved (P<0.001). The improvement in the time spent at the target SpO2 was 56.3%. The ICERs indicate that FreeO2 technology is more cost-effective than manual oxygen titration with a savings of -$C96.91 per percentage point of time spent at the target SpO2 (95% CI -301.26 to 116.96).
Conclusion: FreeO2 technology could significantly enhance the efficiency of the health system by reducing per-patient costs at 180 days. A study with a larger patient sample needs to be carried out to confirm these preliminary results.
Trial registration number: NCT01393015; Post-results.
Keywords: bootstrap; canada; copd; cost-effectiveness; freeo2; oxygen-titration.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: FL is the coinventor of the FreeO2 system and cofounder of Oxynov, the firm that developed and productionised the FreeO2 system for marketing. The Fonds de Recherche en Santé du Québec contributes to Dr François Lellouche salary for research activities (clinical research scholar) and to the research assistant’s salary (clinical research grant). FM holds a GlaxoSmithKline/Canadian Institutes of Health Research chair on COPD at Laval University. FM participates in Innovair, a company that owns shares in OxyNov, the owner of the FreeO2 device.
Figures
References
-
- World Health Organization. Chronic obstructive pulmonary disease (COPD). 2016. http://www.who.int/respiratory/copd/en/ (accessed 23 Nov 2016).
-
- Statistique Canada. Enquête sur la santé dans les collectivités canadiennes. 2010. http://www.cadretravailpulmonaire.ca/santerespiratoireauCanada/ (accessed 23 Nov 2016).
-
- Agence de la santé publique du Canada. Faits saillants sur la maladie pulmonaire obstructive chronique (MPOC). 2011. http://www.phac-aspc.gc.ca/cd-mc/publications/copd-mpoc/ff-rr-2011-fra.php (accessed 23 Nov 2016).
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical