

A systematic review and meta-analysis: Association between MGMT hypermethylation and the clinicopathological characteristics of non-small-cell lung carcinoma
- PMID: 29362385
- PMCID: PMC5780517
- DOI: 10.1038/s41598-018-19949-z
A systematic review and meta-analysis: Association between MGMT hypermethylation and the clinicopathological characteristics of non-small-cell lung carcinoma
Abstract
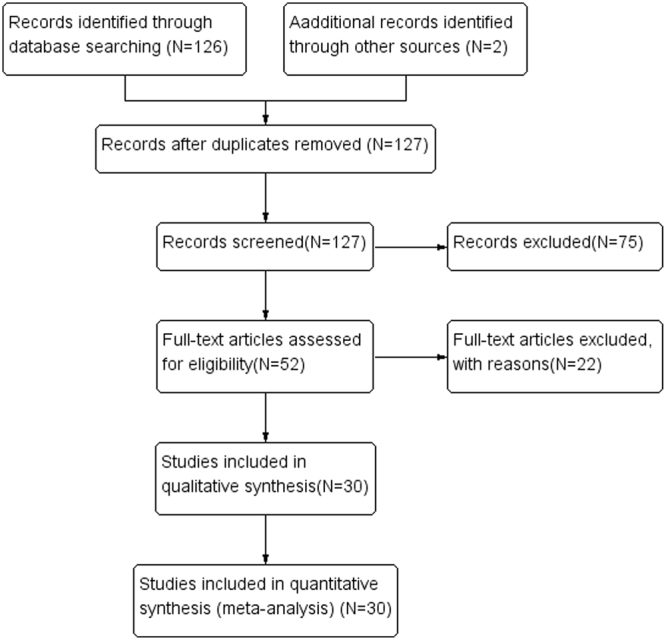
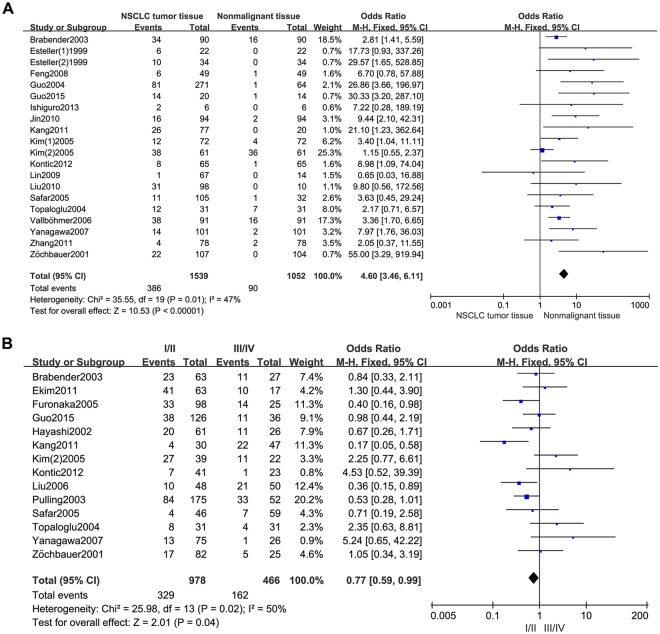
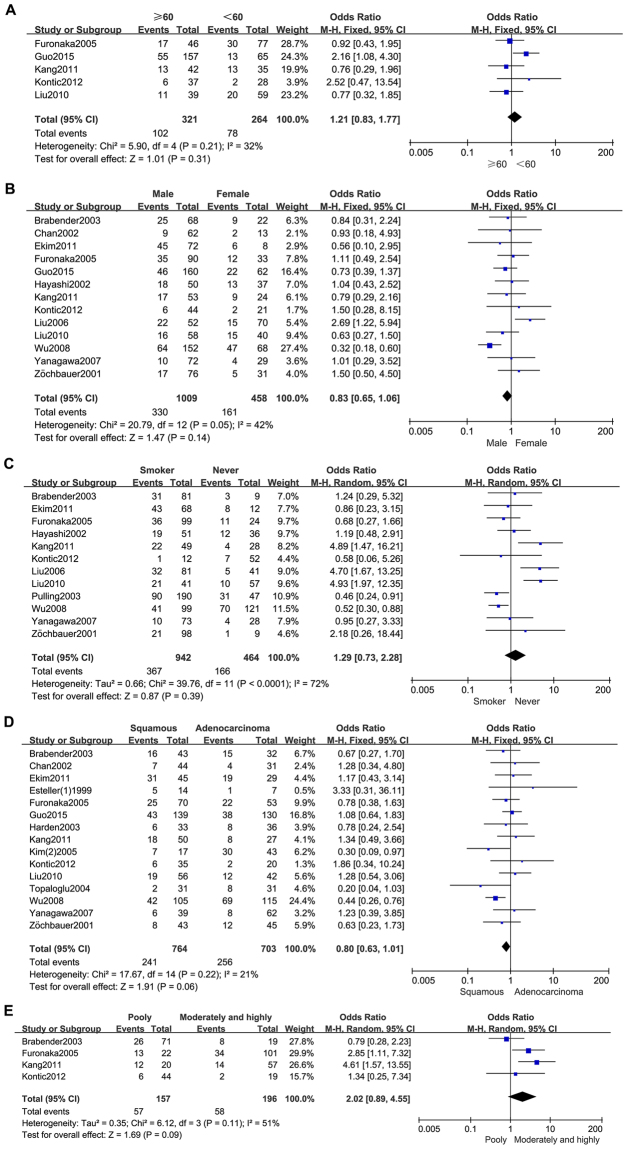
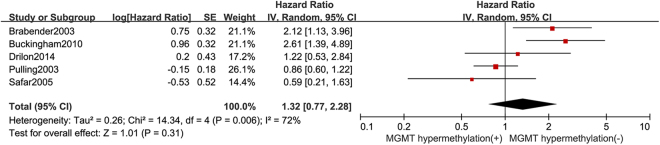
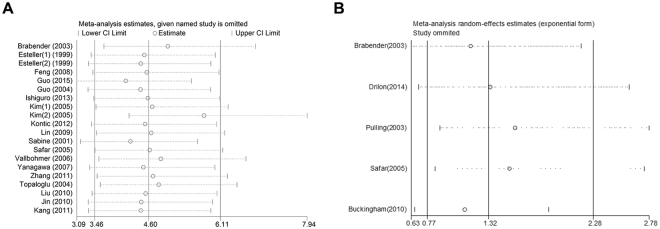
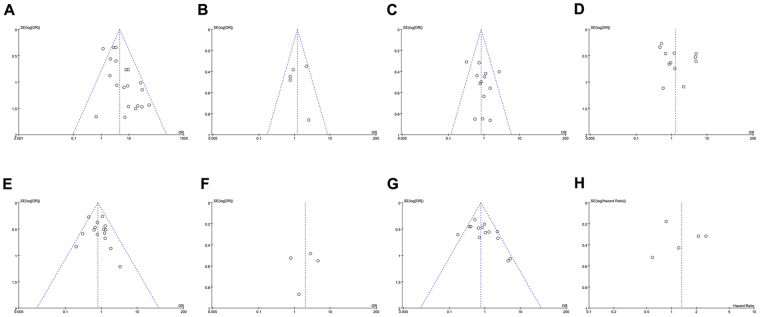
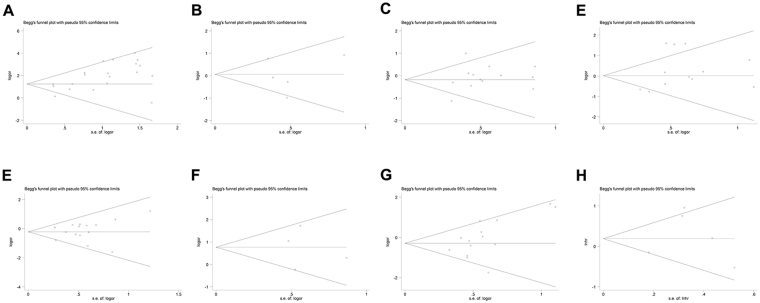
The relationship between O-6-methylguanine-DNA methyltransferase (MGMT) promoter methylation and clinicopathological characteristics of non-small-cell lung carcinoma (NSCLC) has remained controversial and unclear. Therefore, in this study we have undertaken a systematic review and meta-analysis of relevant studies to quantitatively investigate this association. We identified 30 eligible studies investigating 2714 NSCLC patients. The relationship between MGMT hypermethylation and NSCLC was identified based on 20 studies, including 1539 NSCLC patient tissue and 1052 normal and adjacent tissue samples (OR = 4.60, 95% CI = 3.46~6.11, p < 0.00001). MGMT methylation varied with ethnicity (caucasian: OR = 4.56, 95% CI = 2.63~7.92, p < 0.00001; asian: OR = 5.18, 95% CI = 2.03~13.22, p = 0.0006) and control style (autologous: OR = 4.44, 95% CI = 3.32~5.92, p < 0.00001; heterogeneous: OR = 9.05, 95% CI = 1.79~45.71, p = 0.008). In addition, MGMT methylation was observed to be specifically associated with NSCLC clinical stage, and not with age, sex, smoking, pathological types, and differentiation status. Also MGMT methylation did not impact NSCLC patients survival (HR = 1.32, 95% CI = 0.77~2.28, p = 0.31). Our study provided clear evidence about the association of MGMT hypermethylation with increased risk of NSCLC.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
