

The Difficult Evolution of Intensive Cardiac Care Units: An Overview of the BLITZ-3 Registry and Other Italian Surveys
- PMID: 29362712
- PMCID: PMC5736902
- DOI: 10.1155/2017/6025470
The Difficult Evolution of Intensive Cardiac Care Units: An Overview of the BLITZ-3 Registry and Other Italian Surveys
Abstract
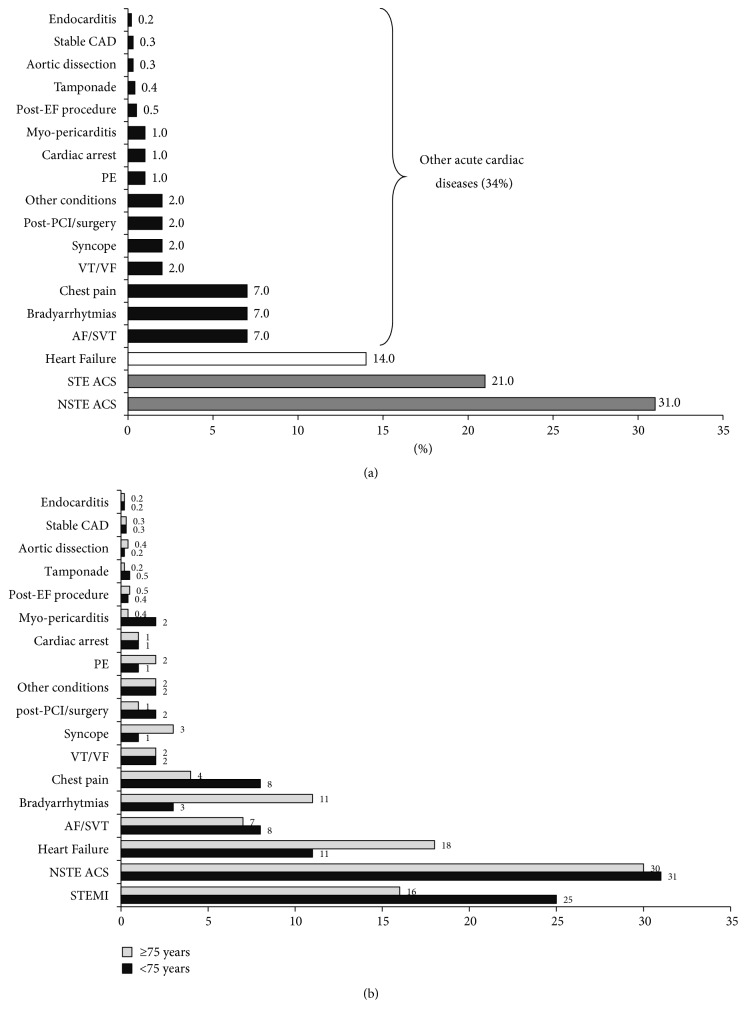
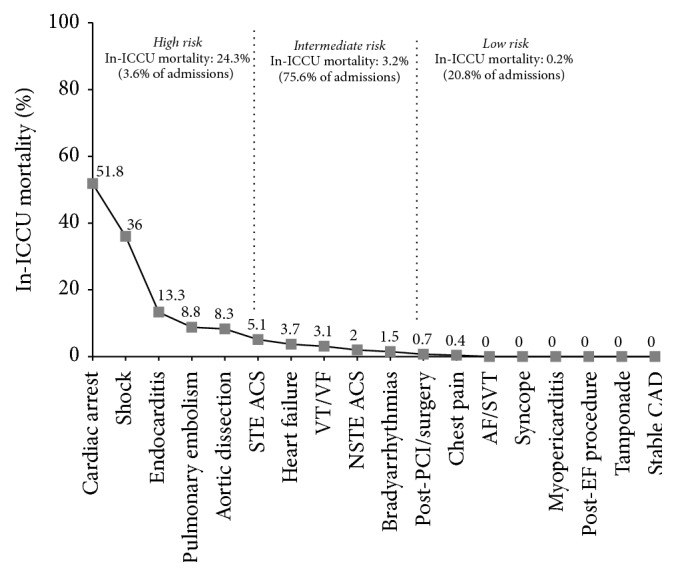
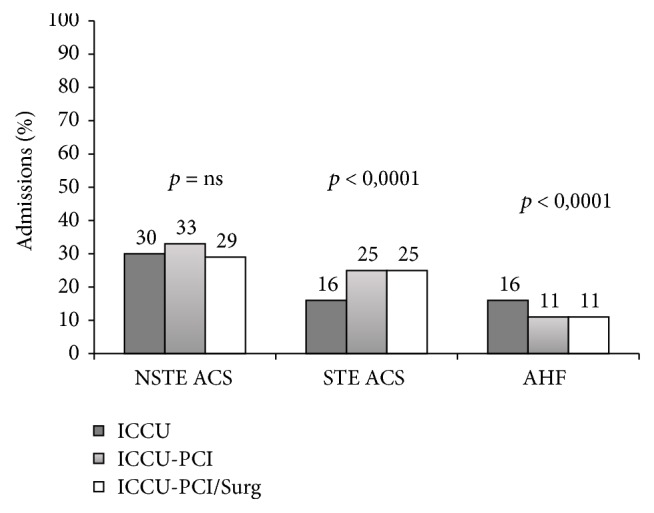
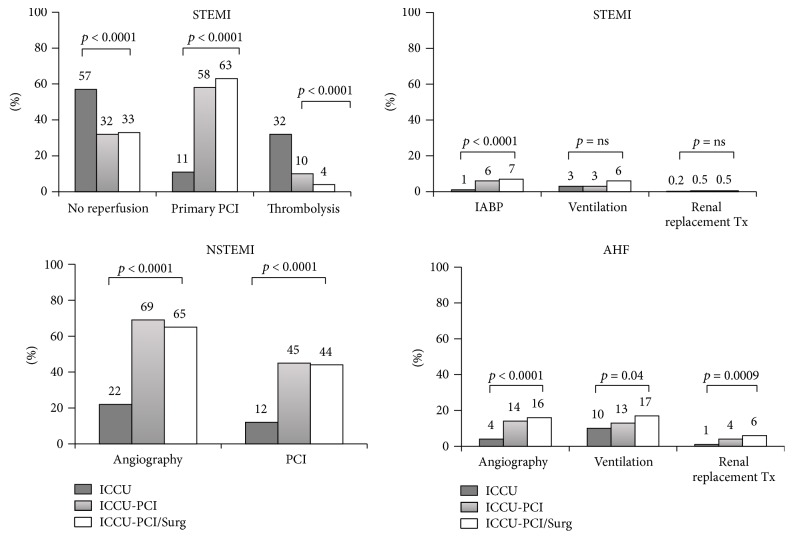
Coronary care units, initially developed to treat acute myocardial infarction, have moved to the care of a broader population of acute cardiac patients and are currently defined as Intensive Cardiac Care Units (ICCUs). However, very limited data are available on such evolution. Since 2008, in Italy, several surveys have been designed to assess ICCUs' activities. The largest and most comprehensive of these, the BLITZ-3 Registry, observed that patients admitted are mainly elderly males and suffer from several comorbidities. Direct admission to ICCUs through the Emergency Medical System was rather rare. Acute coronary syndromes (ACS) account for more than half of the discharge diagnoses. However, numbers of acute heart failure (AHF) admissions are substantial. Interestingly, age, resources availability, and networking have a strong influence on ICCUs' epidemiology and activities. In fact, while patients with ACS concentrate in ICCUs with interventional capabilities, older patients with AHF or non-ACS, non-AHF cardiac diseases prevail in peripheral ICCUs. In conclusion, although ACS is still the core business of ICCUs, aging, comorbidities, increasing numbers of non-ACS, technological improvements, and resources availability have had substantial effects on epidemiology and activities of ICCUs. The Italian surveys confirm these changes and call for a substantial update of ICCUs' organization and competences.
Figures
Similar articles
-
Epidemiology and patterns of care of patients admitted to Italian Intensive Cardiac Care units: the BLITZ-3 registry.J Cardiovasc Med (Hagerstown). 2010 Jun;11(6):450-61. doi: 10.2459/JCM.0b013e328335233e. J Cardiovasc Med (Hagerstown). 2010. PMID: 19952775
-
[Distribution and appropriateness of hospital admissions, resource utilization in the Italian intensive cardiac care units. The BLITZ-3 study].G Ital Cardiol (Rome). 2011 Jan;12(1):23-30. G Ital Cardiol (Rome). 2011. PMID: 21428024 Italian.
-
Elderly patients with acute coronary syndromes admitted to Italian intensive cardiac care units: a Blitz-3 Registry sub-analysis.J Cardiovasc Med (Hagerstown). 2012 Mar;13(3):165-74. doi: 10.2459/JCM.0b013e3283515be3. J Cardiovasc Med (Hagerstown). 2012. PMID: 22306786
-
Characteristics of Intensive Care in Patients Hospitalized for Heart Failure in Europe.Heart Fail Clin. 2015 Oct;11(4):647-56. doi: 10.1016/j.hfc.2015.07.005. Heart Fail Clin. 2015. PMID: 26462104 Review.
-
[Clinical competence of the cardiologists working in coronary care units].G Ital Cardiol (Rome). 2007 May;8(5 Suppl 1):16S-24S. G Ital Cardiol (Rome). 2007. PMID: 17649869 Review. Italian.
Cited by
-
Strategies to Lower In-Hospital Mortality in STEMI Patients with Primary PCI: Analysing Two Years Data from a High-Volume Interventional Centre.J Interv Cardiol. 2019 Oct 1;2019:3402081. doi: 10.1155/2019/3402081. eCollection 2019. J Interv Cardiol. 2019. PMID: 31772524 Free PMC article.
-
Impact of COVID-19 Pandemic on STEMI Networks in Central Romania.Life (Basel). 2021 Sep 24;11(10):1004. doi: 10.3390/life11101004. Life (Basel). 2021. PMID: 34685376 Free PMC article.
-
Morbidity pattern and outcome of patients admitted in a coronary care unit: a report from a secondary hospital in southern region, Saudi Arabia.J Community Hosp Intern Med Perspect. 2018 Aug 23;8(4):191-194. doi: 10.1080/20009666.2018.1500421. eCollection 2018. J Community Hosp Intern Med Perspect. 2018. PMID: 30181824 Free PMC article.
References
-
- Morrow D. A., Fang J. C., Fintel D. J., et al. Evolution of critical care cardiology: transformation of the cardiovascular intensive care unit and the emerging need for new medical staffing and training models: a scientific statement from the American Heart Association. Circulation. 2012;126(11):1408–1428. doi: 10.1161/CIR.0b013e31826890b0. - DOI - PubMed
-
- Gardini E., Caravita L., Ottani F., Ferrini D., Galvani M. Coronary care units: who to admit and how long. Giornale Italiano Di Cardiologia. 2007;8(supplement 1):5S–11S. - PubMed
-
- Lettino M., Vrints C. Acute cardiovascular care IV. European Heart Journal. 2013;34(35):2717–2718. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
