

Effect of Prolonged Exposure Therapy Delivered Over 2 Weeks vs 8 Weeks vs Present-Centered Therapy on PTSD Symptom Severity in Military Personnel: A Randomized Clinical Trial
- PMID: 29362795
- PMCID: PMC5833566
- DOI: 10.1001/jama.2017.21242
Effect of Prolonged Exposure Therapy Delivered Over 2 Weeks vs 8 Weeks vs Present-Centered Therapy on PTSD Symptom Severity in Military Personnel: A Randomized Clinical Trial
Erratum in
-
Error in Dropout Number for Spaced Prolonged Exposure Therapy.JAMA. 2018 Aug 21;320(7):724. doi: 10.1001/jama.2018.11067. JAMA. 2018. PMID: 30140857 Free PMC article. No abstract available.
Abstract
Importance: Effective and efficient treatment is needed for posttraumatic stress disorder (PTSD) in active duty military personnel.
Objective: To examine the effects of massed prolonged exposure therapy (massed therapy), spaced prolonged exposure therapy (spaced therapy), present-centered therapy (PCT), and a minimal-contact control (MCC) on PTSD severity.
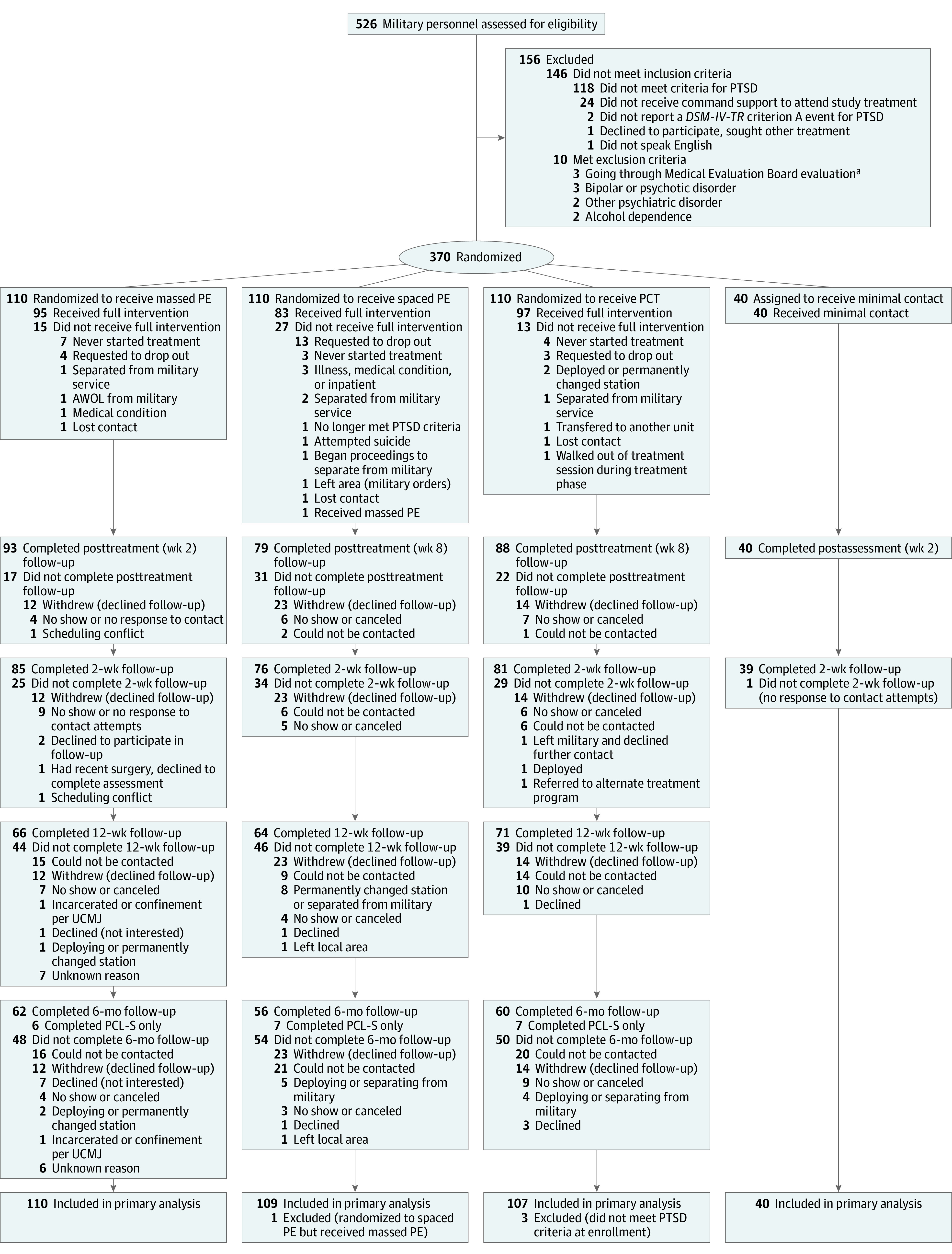
Design, setting, and participants: Randomized clinical trial conducted at Fort Hood, Texas, from January 2011 through July 2016 and enrolling 370 military personnel with PTSD who had returned from Iraq, Afghanistan, or both. Final follow-up was July 11, 2016.
Interventions: Prolonged exposure therapy, cognitive behavioral therapy involving exposure to trauma memories/reminders, administered as massed therapy (n = 110; 10 sessions over 2 weeks) or spaced therapy (n = 109; 10 sessions over 8 weeks); PCT, a non-trauma-focused therapy involving identifying/discussing daily stressors (n = 107; 10 sessions over 8 weeks); or MCC, telephone calls from therapists (n = 40; once weekly for 4 weeks).
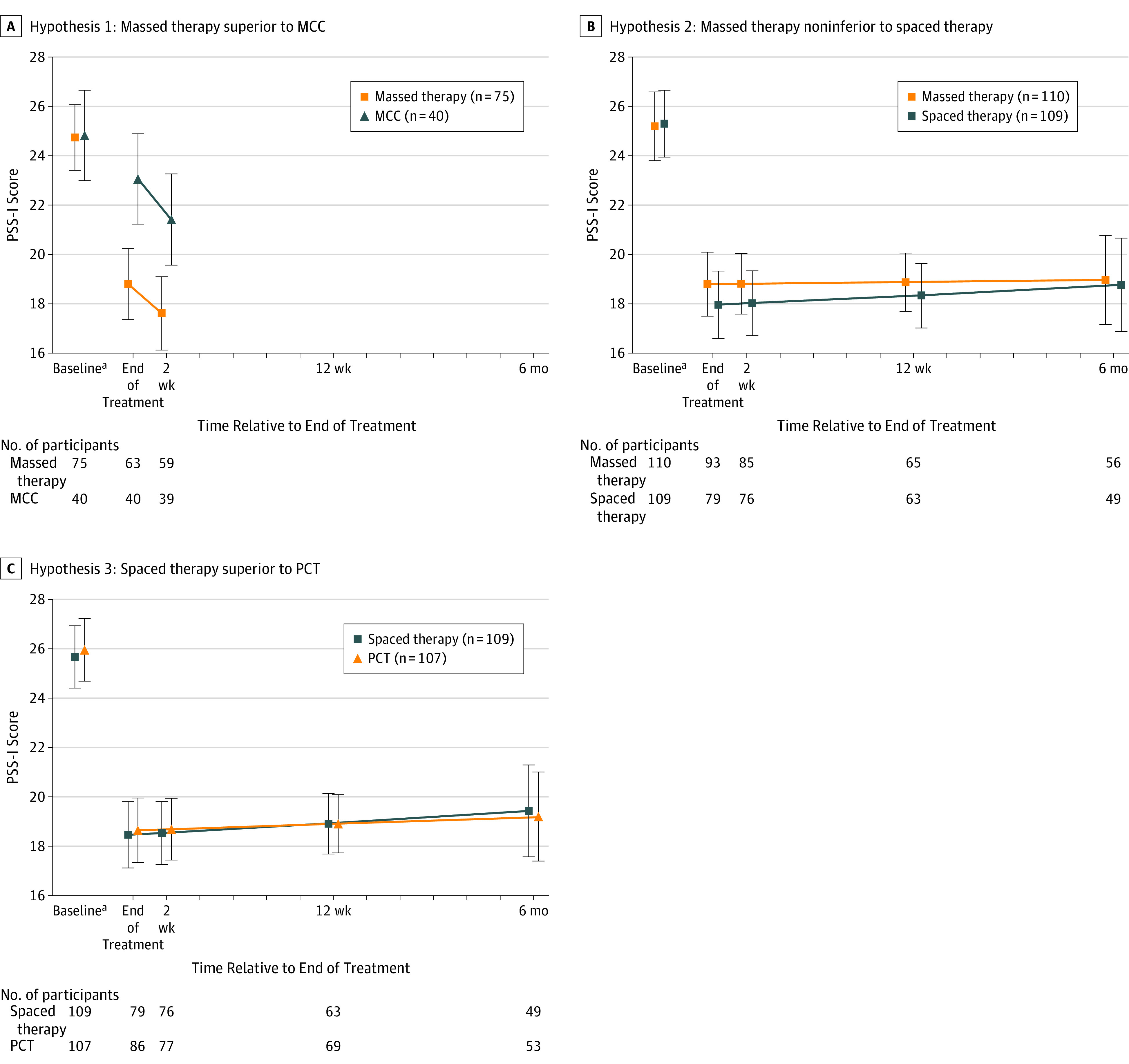
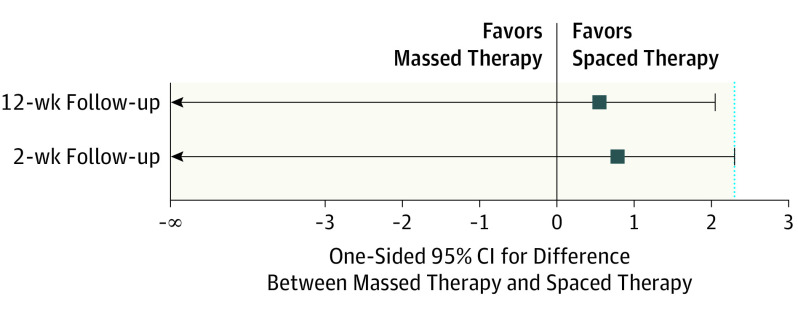
Main outcomes and measures: Outcomes were assessed before and after treatment and at 2-week, 12-week, and 6-month follow-up. Primary outcome was interviewer-assessed PTSD symptom severity, measured by the PTSD Symptom Scale-Interview (PSS-I; range, 0-51; higher scores indicate greater PTSD severity; MCID, 3.18), used to assess efficacy of massed therapy at 2 weeks posttreatment vs MCC at week 4; noninferiority of massed therapy vs spaced therapy at 2 weeks and 12 weeks posttreatment (noninferiority margin, 50% [2.3 points on PSS-I, with 1-sided α = .05]); and efficacy of spaced therapy vs PCT at posttreatment.
Results: Among 370 randomized participants, data were analyzed for 366 (mean age, 32.7 [SD, 7.3] years; 44 women [12.0%]; mean baseline PSS-I score, 25.49 [6.36]), and 216 (59.0%) completed the study. At 2 weeks posttreatment, mean PSS-I score was 17.62 (mean decrease from baseline, 7.13) for massed therapy and 21.41 (mean decrease, 3.43) for MCC (difference in decrease, 3.70 [95% CI,0.72 to 6.68]; P = .02). At 2 weeks posttreatment, mean PSS-I score was 18.03 for spaced therapy (decrease, 7.29; difference in means vs massed therapy, 0.79 [1-sided 95% CI, -∞ to 2.29; P = .049 for noninferiority]) and at 12 weeks posttreatment was 18.88 for massed therapy (decrease, 6.32) and 18.34 for spaced therapy (decrease, 6.97; difference, 0.55 [1-sided 95% CI, -∞ to 2.05; P = .03 for noninferiority]). At posttreatment, PSS-I scores for PCT were 18.65 (decrease, 7.31; difference in decrease vs spaced therapy, 0.10 [95% CI, -2.48 to 2.27]; P = .93).
Conclusions and relevance: Among active duty military personnel with PTSD, massed therapy (10 sessions over 2 weeks) reduced PTSD symptom severity more than MCC at 2-week follow-up and was noninferior to spaced therapy (10 sessions over 8 weeks), and there was no significant difference between spaced therapy and PCT. The reductions in PTSD symptom severity with all treatments were relatively modest, suggesting that further research is needed to determine the clinical importance of these findings.
Trial registration: clinicaltrials.gov Identifier: NCT01049516.
Conflict of interest statement
Figures
Comment in
-
A Window Into the Evolution of Trauma-Focused Psychotherapies for Posttraumatic Stress Disorder.JAMA. 2018 Jan 23;319(4):343-345. doi: 10.1001/jama.2017.21880. JAMA. 2018. PMID: 29362777 No abstract available.
-
Motivation to Participate in PTSD Research.JAMA. 2018 Jun 19;319(23):2439-2440. doi: 10.1001/jama.2018.4326. JAMA. 2018. PMID: 29922819 No abstract available.
-
First-line Psychotherapies for Military-Related PTSD.JAMA. 2020 Feb 18;323(7):656-657. doi: 10.1001/jama.2019.20825. JAMA. 2020. PMID: 31999301 No abstract available.
References
-
- Hoge CW, Terhakopian A, Castro CA, Messer SC, Engel CC. Association of posttraumatic stress disorder with somatic symptoms, health care visits, and absenteeism among Iraq war veterans. Am J Psychiatry. 2007;164(1):150-153. - PubMed
-
- Milliken CS, Auchterlonie JL, Hoge CW. Longitudinal assessment of mental health problems among active and reserve component soldiers returning from the Iraq war. JAMA. 2007;298(18):2141-2148. - PubMed
-
- Gates MA, Holowka DW, Vasterling JJ, Keane TM, Marx BP, Rosen RC. Posttraumatic stress disorder in veterans and military personnel. Psychol Serv. 2012;9(4):361-382. - PubMed
-
- Asnaani A, Reddy MK, Shea MT. The impact of PTSD symptoms on physical and mental health functioning in returning veterans. J Anxiety Disord. 2014;28(3):310-317. - PubMed
-
- Kessler RC. Posttraumatic stress disorder: the burden to the individual and to society. J Clin Psychiatry. 2000;61(suppl 5):4-12. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
