

The impact of cerclage in twin pregnancies on preterm birth rate before 32 weeks
- PMID: 29363371
- PMCID: PMC6251764
- DOI: 10.1080/14767058.2018.1427719
The impact of cerclage in twin pregnancies on preterm birth rate before 32 weeks
Abstract
Purpose: To evaluate whether cerclage in twins reduces the rate of spontaneous preterm birth <32 weeks when compared to expectant management.
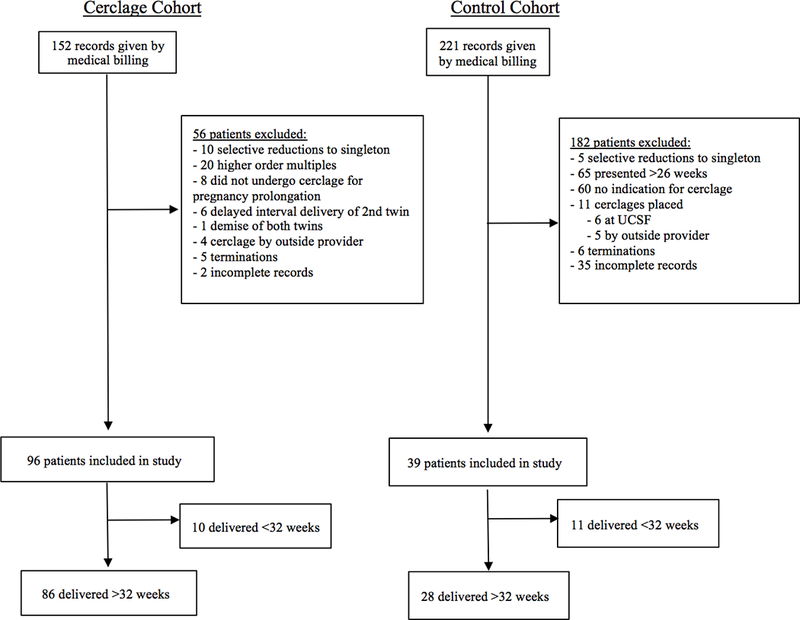
Methods: This is a retrospective cohort study of twin pregnancies with the following indications for cerclage from two institutions: history of prior preterm birth, ultrasound-identified short cervix ≤2.5 cm, and cervical dilation ≥1.0 cm. The "cerclage" cohort received a cerclage from a single provider at a single institution from 2003-2016. The "no cerclage" group included all patients with similar indications that were expectantly managed from 2010-2015, at a second institution where cerclages are routinely not performed in twin pregnancies. The primary outcome was the rate of spontaneous preterm birth at <32 weeks. Secondary outcomes were the rates of spontaneous and overall (including medically indicated) preterm births at <32 weeks, < 34 weeks, and <36 weeks, chorioamnionitis, birth weight, and neonatal mortality within 30 days of life. We also performed a planned subgroup analysis stratified by cerclage indication.
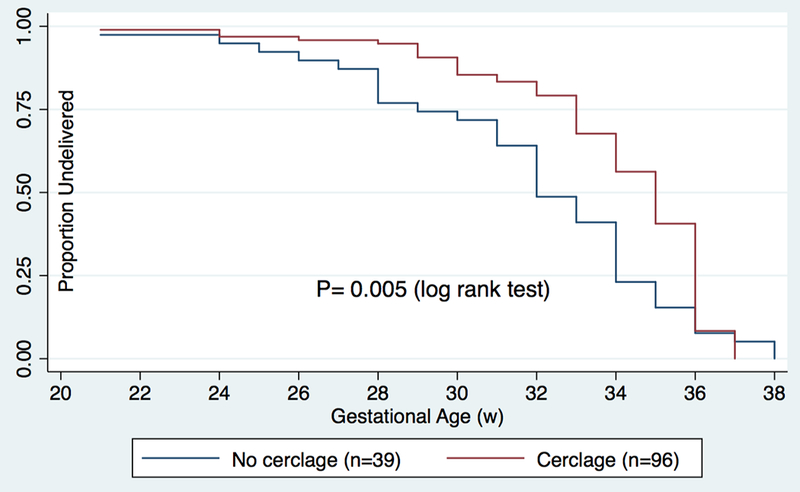
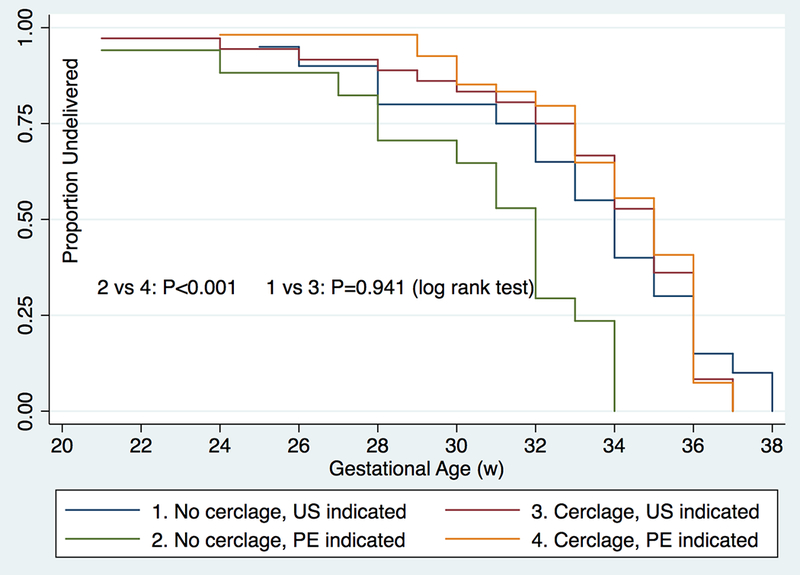
Results: In all, 135 women were included in two cohorts: cerclage (n = 96) or no cerclage (n = 39). The rates of spontaneous preterm birth <32 weeks were 10.4% (n = 10) with cerclage versus 28.2% (n = 11) without cerclage (OR 0.23, CI 0.08-0.70, p = .017). After adjusting for cerclage indication, clinical history, age, chorionicity, insurance type, race, BMI, in-vitro fertilization, and multifetal reduction, there remained a significant reduction in the cerclage group of spontaneous preterm birth <32 weeks (adjusted odds ratio (aOR) 0.24, CI 0.06-0.90, p = .035), spontaneous preterm birth <36 weeks (aOR 0.34, CI 0.04-0.81, p = .013) as well as in overall preterm birth <32 weeks (aOR 0.31, CI 0.1-0.86, p = .018), and overall preterm birth <36 weeks (aOR 0.37, CI 0.10-0.84, p = .030). When stratified by short cervix or cervical dilation in the cerclage versus no cerclage groups, there was a significant decrease in spontaneous preterm birth <32 weeks in the cerclage group with cervical dilation (11.1 versus 41.2%, p = .01) but not in the cerclage group with short cervix only, even for cervical length <1.5 cm. Pregnancy latency was 91 days in the cerclage group versus 57 days in the no cerclage group (p = .001), with a median gestational age at delivery of 35 versus 32 weeks (p = .002). There was no increase in chorioamnionitis in the cerclage group. Furthermore, there was a significant increase in birth weight (median 2278 versus 1665 g, p < .001) and decrease in perinatal death <30 days (1.6 versus 12.9%, p = .001).
Conclusions: Cerclage in twin pregnancies significantly decreased the rate of spontaneous preterm birth <32 weeks compared to expectant management. However, when stratified by cerclage indication, this decrease in primary outcome only remained significant in the group with cervical dilation.
Keywords: Prematurity; cervical insufficiency; multiple gestation; rescue; short cervix.
Conflict of interest statement
Figures
References
-
- Martin JA, Hamilton BE, Osterman MJK, Curtin SC, Mathews TJ. National vital statistics reports. Births: final data for 2013. 2015 - PubMed
-
- Practice Bulletin No. 171: Management of Preterm Labor. The American College of Obstetricians and Gynecologists 2016;128:931–933. - PubMed
-
- Dor J, Shalev J, Mashiach S, Blankstein J, Serr DM. Elective cervical suture of twin pregnancies diagnosed ultrasonically in the first trimester following induced ovulation. Gynecol Obstet Invest 1982;13:55e60. - PubMed
-
- Rust OA, Atlas RO, Reed J, van Gaalen J, Balducci J. Revisiting the short cervix detected by transvaginal ultrasound in the second trimester: why cerclage therapy may not help. Am J Obstet Gynecol 2001;185: - PubMed
-
- Althuisius SM, Dekker GA, Hummel P, Bekedam DJ, van Geijn HP. Final results of the Cervical Incompetence Prevention Randomized Cerclage Trial (CIPRACT): therapeutic cerclage with bed rest versus bed rest alone. Am J Obstet Gynecol 2001;185:1106e12. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical