

Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging
- PMID: 29364767
- PMCID: PMC6590673
- DOI: 10.1056/NEJMoa1713973
Thrombectomy for Stroke at 6 to 16 Hours with Selection by Perfusion Imaging
Abstract
Background: Thrombectomy is currently recommended for eligible patients with stroke who are treated within 6 hours after the onset of symptoms.
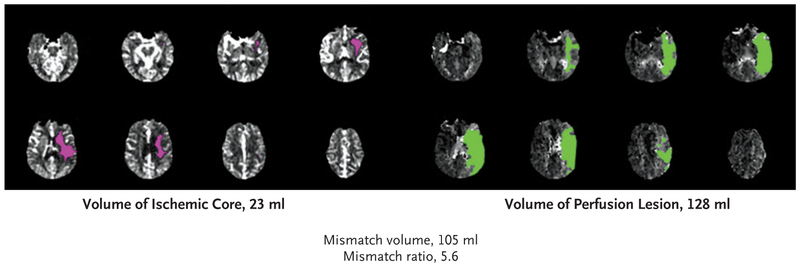
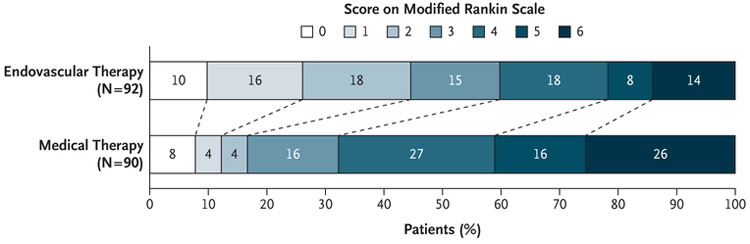
Methods: We conducted a multicenter, randomized, open-label trial, with blinded outcome assessment, of thrombectomy in patients 6 to 16 hours after they were last known to be well and who had remaining ischemic brain tissue that was not yet infarcted. Patients with proximal middle-cerebral-artery or internal-carotid-artery occlusion, an initial infarct size of less than 70 ml, and a ratio of the volume of ischemic tissue on perfusion imaging to infarct volume of 1.8 or more were randomly assigned to endovascular therapy (thrombectomy) plus standard medical therapy (endovascular-therapy group) or standard medical therapy alone (medical-therapy group). The primary outcome was the ordinal score on the modified Rankin scale (range, 0 to 6, with higher scores indicating greater disability) at day 90.
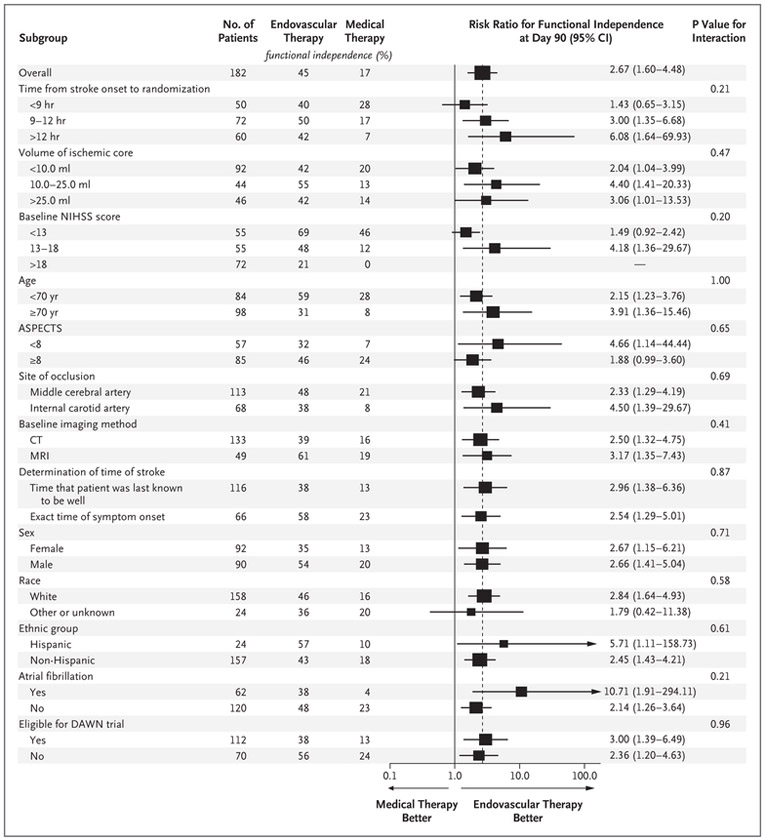
Results: The trial was conducted at 38 U.S. centers and terminated early for efficacy after 182 patients had undergone randomization (92 to the endovascular-therapy group and 90 to the medical-therapy group). Endovascular therapy plus medical therapy, as compared with medical therapy alone, was associated with a favorable shift in the distribution of functional outcomes on the modified Rankin scale at 90 days (odds ratio, 2.77; P<0.001) and a higher percentage of patients who were functionally independent, defined as a score on the modified Rankin scale of 0 to 2 (45% vs. 17%, P<0.001). The 90-day mortality rate was 14% in the endovascular-therapy group and 26% in the medical-therapy group (P=0.05), and there was no significant between-group difference in the frequency of symptomatic intracranial hemorrhage (7% and 4%, respectively; P=0.75) or of serious adverse events (43% and 53%, respectively; P=0.18).
Conclusions: Endovascular thrombectomy for ischemic stroke 6 to 16 hours after a patient was last known to be well plus standard medical therapy resulted in better functional outcomes than standard medical therapy alone among patients with proximal middle-cerebral-artery or internal-carotid-artery occlusion and a region of tissue that was ischemic but not yet infarcted. (Funded by the National Institute of Neurological Disorders and Stroke; DEFUSE 3 ClinicalTrials.gov number, NCT02586415 .).
Figures
Comment in
-
Stroke: Expanding the thrombectomy time window after stroke.Nat Rev Neurol. 2018 Mar;14(3):128. doi: 10.1038/nrneurol.2018.15. Epub 2018 Feb 9. Nat Rev Neurol. 2018. PMID: 29422645 No abstract available.
-
Reperfusion in the brain: is time important? The DAWN and DEFUSE-3 trials.Cardiovasc Res. 2018 Apr 1;114(5):e28-e29. doi: 10.1093/cvr/cvy053. Cardiovasc Res. 2018. PMID: 29590391 No abstract available.
-
In perfusion imaging-selected acute ischemic stroke, thrombectomy at 6 to 16 hours improved functional outcomes.Ann Intern Med. 2018 Apr 17;168(8):JC42. doi: 10.7326/ACPJC-2018-168-8-042. Ann Intern Med. 2018. PMID: 29677249 No abstract available.
-
Thrombectomy for Stroke with Selection by Perfusion Imaging.N Engl J Med. 2018 May 10;378(19):1849. doi: 10.1056/NEJMc1803856. N Engl J Med. 2018. PMID: 29745632 No abstract available.
-
MRI-Guided Intravenous Alteplase for Stroke - Still Stuck in Time.N Engl J Med. 2018 Aug 16;379(7):682-683. doi: 10.1056/NEJMe1805796. Epub 2018 May 16. N Engl J Med. 2018. PMID: 29766752 No abstract available.
References
-
- Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet 2016;387: 1723–31. - PubMed
-
- Powers WJ, Derdeyn CP, Biller J, et al. 2015 American Heart Association/American Stroke Association focused update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular Treatment: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2015; 46:3020–35. - PubMed
-
- Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med 2018;378:11–21. - PubMed
-
- Albers GW, Goyal M, Jahan R, et al. Ischemic core and hypoperfusion volumes predict infarct size in SWIFT PRIME. Ann Neurol 2016;79:76–89. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical