

Consequences of the 340B Drug Pricing Program
- PMID: 29365282
- PMCID: PMC6073067
- DOI: 10.1056/NEJMsa1706475
Consequences of the 340B Drug Pricing Program
Abstract
Background: The 340B Drug Pricing Program entitles qualifying hospitals to discounts on outpatient drugs, increasing the profitability of drug administration. By tying the program eligibility of hospitals to their Disproportionate Share Hospital (DSH) adjustment percentage, which reflects the proportion of hospitalized patients who are low-income, the program is intended to expand resources for underserved populations but provides no direct incentives for hospitals to use financial gains to enhance care for low-income patients.
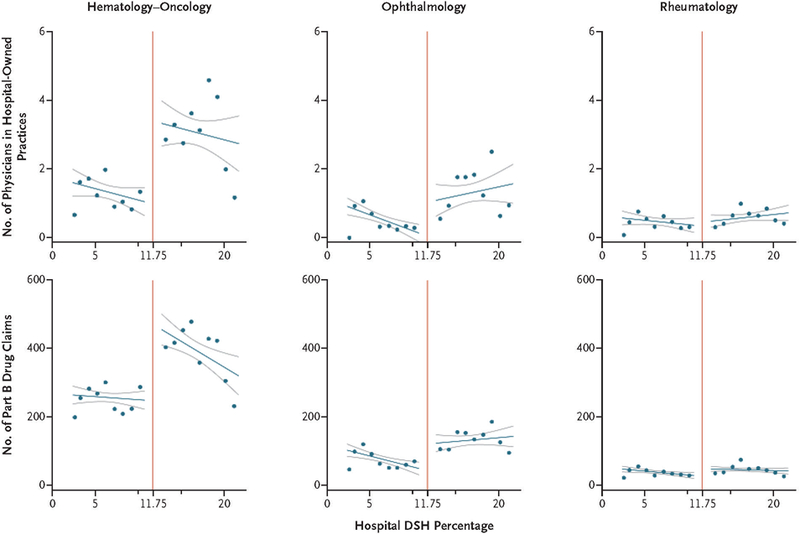
Methods: We used Medicare claims and a regression-discontinuity design, taking advantage of the threshold for program eligibility among general acute care hospitals (DSH percentage, >11.75%), to isolate the effects of the program on hospital-physician consolidation (i.e., acquisition of physician practices or employment of physicians by hospitals) and on the outpatient administration of parenteral drugs by hospital-owned facilities in three specialties in which parenteral drugs are frequently used. For low-income patients, we also assessed the effects of the program on the provision of care by hospitals and on mortality.
Results: Hospital eligibility for the 340B Program was associated with 2.3 more hematologist-oncologists practicing in facilities owned by the hospital, or 230% more hematologist-oncologists than expected in the absence of the program (P=0.02), and with 0.9 (or 900%) more ophthalmologists per hospital (P=0.08) and 0.1 (or 33%) more rheumatologists per hospital (P=0.84). Program eligibility was associated with significantly higher numbers of parenteral drug claims billed by hospitals for Medicare patients in hematology-oncology (90% higher, P=0.001) and ophthalmology (177% higher, P=0.03) but not rheumatology (77% higher, P=0.12). Program eligibility was associated with lower proportions of low-income patients in hematology-oncology and ophthalmology and with no significant differences in hospital provision of safety-net or inpatient care for low-income groups or in mortality among low-income residents of the hospitals' local service areas.
Conclusions: The 340B Program has been associated with hospital-physician consolidation in hematology-oncology and with more hospital-based administration of parenteral drugs in hematology-oncology and ophthalmology. Financial gains for hospitals have not been associated with clear evidence of expanded care or lower mortality among low-income patients. (Funded by the Agency for Healthcare Research and Quality and others.).
Figures
Comment in
-
Consequences of the 340B Drug Pricing Program.N Engl J Med. 2018 May 24;378(21):2053. doi: 10.1056/NEJMc1802999. N Engl J Med. 2018. PMID: 29792408 No abstract available.
-
Consequences of the 340B Drug Pricing Program.N Engl J Med. 2018 May 24;378(21):2053. doi: 10.1056/NEJMc1802999. N Engl J Med. 2018. PMID: 29792409 No abstract available.
References
-
- Public Health Service Act, 42 U.S.C. § 256b.
-
- Mulcahy AW, Armstrong C, Lewis J, Mattke S. The 340B prescription drug discount program: origins, implementation, and post-reform future Santa Monica, CA: RAND, 2014.
-
- 340B drug pricing program Rockville, MD: Health Resources & Services Administration, November 2017. (https://www.hrsa.gov/opa/).
-
- Overview of the 340B drug pricing program Washington, DC: 340B Health; (http://www.340bhealth.org/340b-resources/340b-program/overview/).
-
- Report to the Congress: overview of the 340B drug pricing program Washington, DC: Medicare Payment Advisory Commission, May 2015. (http://www.medpac.gov/docs/default-source/reports/may-2015-report-to-the...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources