

Preoperative physiotherapy for the prevention of respiratory complications after upper abdominal surgery: pragmatic, double blinded, multicentre randomised controlled trial
- PMID: 29367198
- PMCID: PMC5782401
- DOI: 10.1136/bmj.j5916
Preoperative physiotherapy for the prevention of respiratory complications after upper abdominal surgery: pragmatic, double blinded, multicentre randomised controlled trial
Erratum in
-
Correction for vol. 365, p.BMJ. 2019 Apr 25;365:l1862. doi: 10.1136/bmj.l1862. BMJ. 2019. PMID: 31023704 Free PMC article.
Abstract
Objective: To assess the efficacy of a single preoperative physiotherapy session to reduce postoperative pulmonary complications (PPCs) after upper abdominal surgery.
Design: Prospective, pragmatic, multicentre, patient and assessor blinded, parallel group, randomised placebo controlled superiority trial.
Setting: Multidisciplinary preadmission clinics at three tertiary public hospitals in Australia and New Zealand.
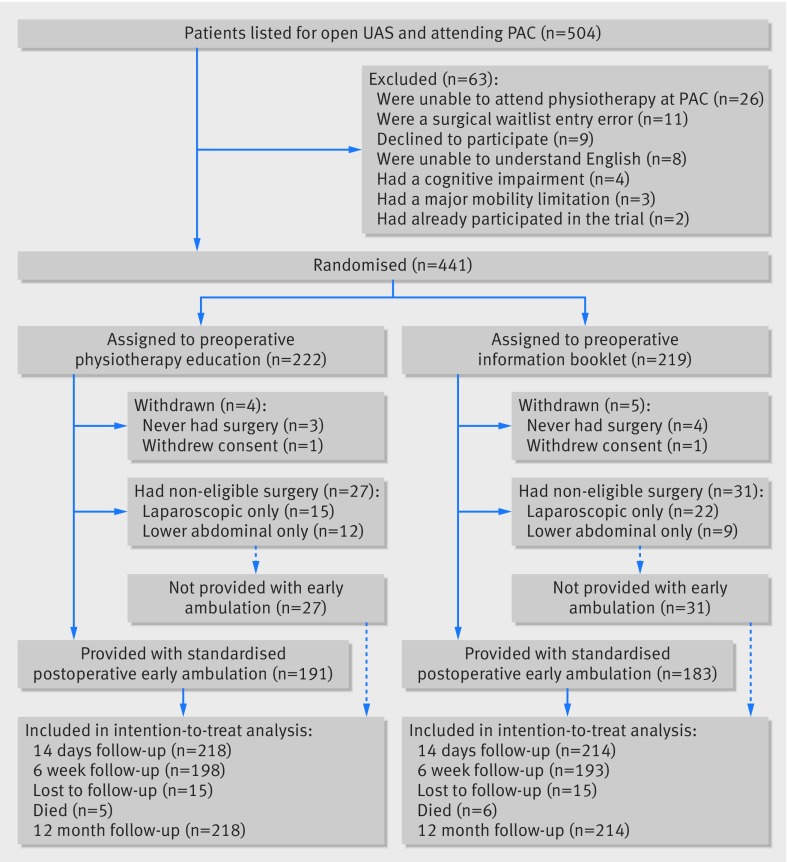
Participants: 441 adults aged 18 years or older who were within six weeks of elective major open upper abdominal surgery were randomly assigned through concealed allocation to receive either an information booklet (n=219; control) or preoperative physiotherapy (n=222; intervention) and followed for 12 months. 432 completed the trial.
Interventions: Preoperatively, participants received an information booklet (control) or an additional 30 minute physiotherapy education and breathing exercise training session (intervention). Education focused on PPCs and their prevention through early ambulation and self directed breathing exercises to be initiated immediately on regaining consciousness after surgery. Postoperatively, all participants received standardised early ambulation, and no additional respiratory physiotherapy was provided.
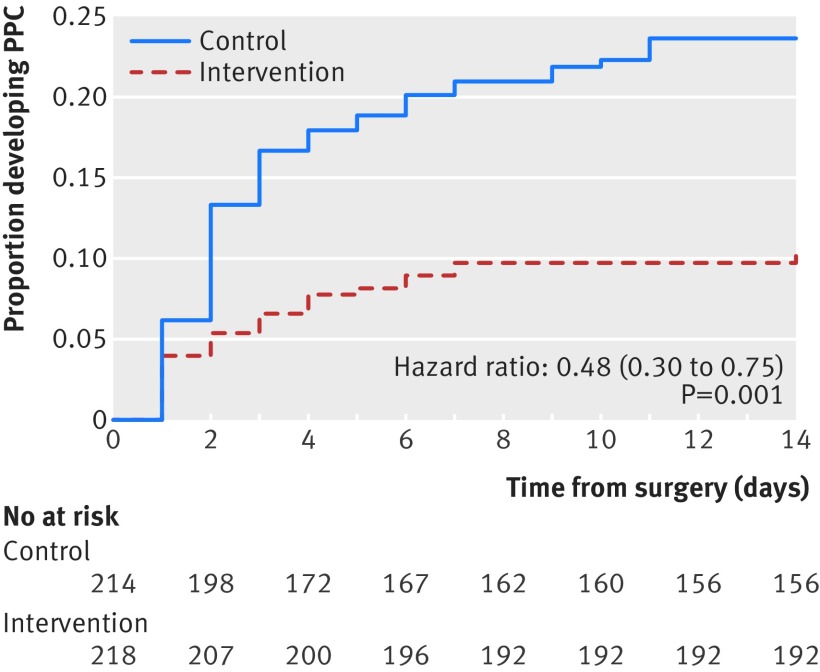
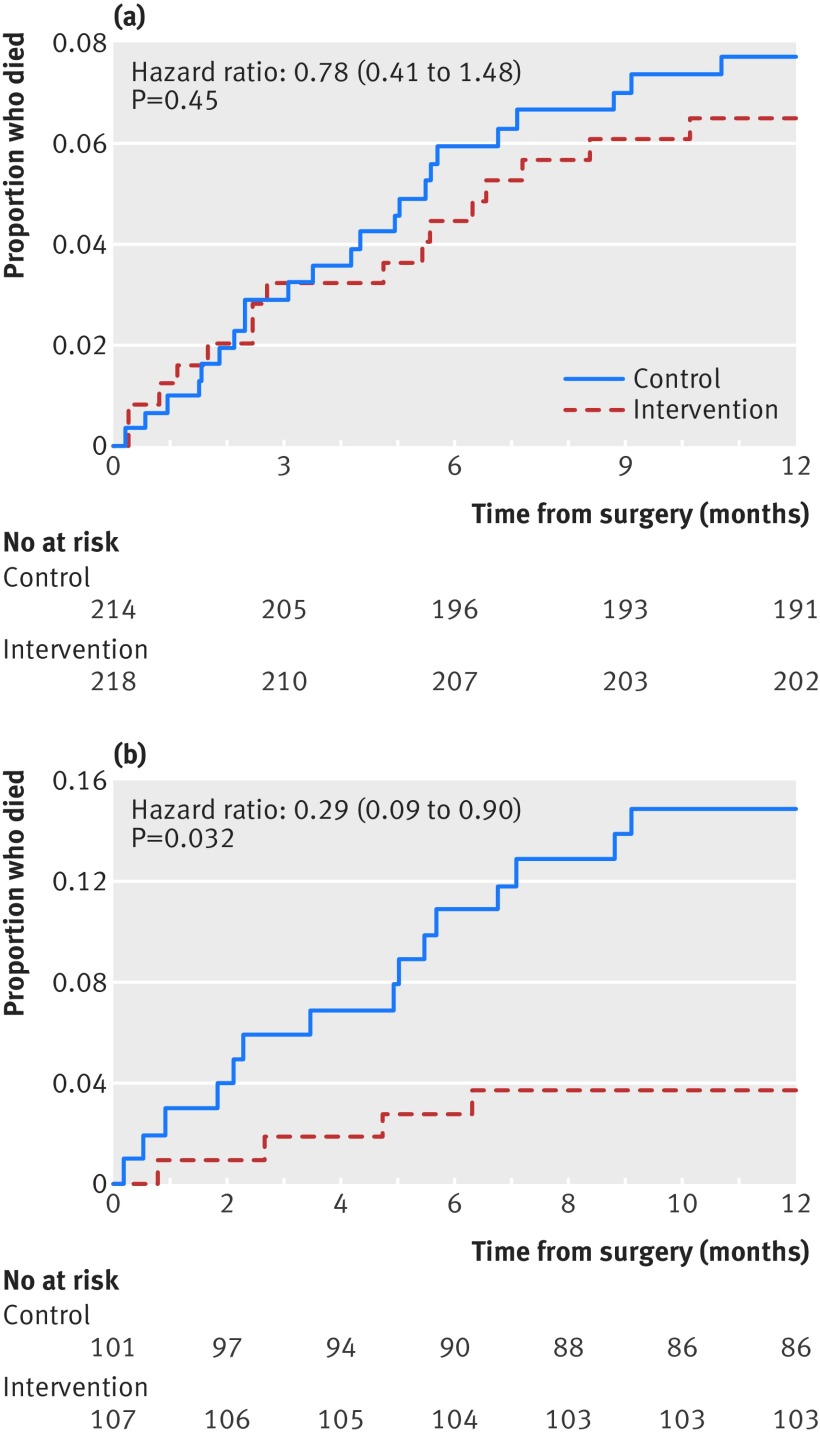
Main outcome measures: The primary outcome was a PPC within 14 postoperative hospital days assessed daily using the Melbourne group score. Secondary outcomes were hospital acquired pneumonia, length of hospital stay, utilisation of intensive care unit services, and hospital costs. Patient reported health related quality of life, physical function, and post-discharge complications were measured at six weeks, and all cause mortality was measured to 12 months.
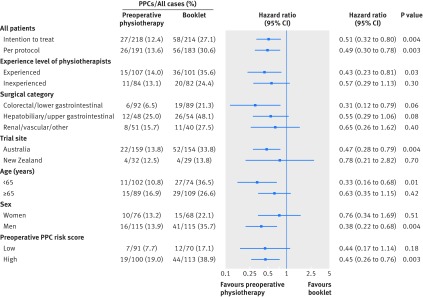
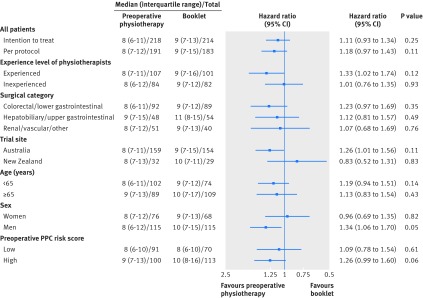
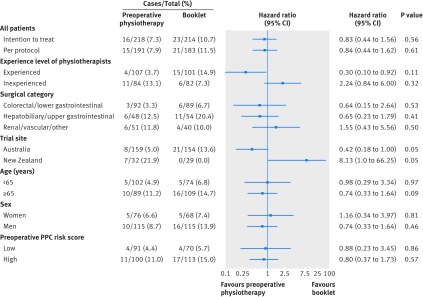
Results: The incidence of PPCs within 14 postoperative hospital days, including hospital acquired pneumonia, was halved (adjusted hazard ratio 0.48, 95% confidence interval 0.30 to 0.75, P=0.001) in the intervention group compared with the control group, with an absolute risk reduction of 15% (95% confidence interval 7% to 22%) and a number needed to treat of 7 (95% confidence interval 5 to 14). No significant differences in other secondary outcomes were detected.
Conclusion: In a general population of patients listed for elective upper abdominal surgery, a 30 minute preoperative physiotherapy session provided within existing hospital multidisciplinary preadmission clinics halves the incidence of PPCs and specifically hospital acquired pneumonia. Further research is required to investigate benefits to mortality and length of stay.
Trial registration: Australian New Zealand Clinical Trials Registry ANZCTR 12613000664741.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare that IB received grants from the Clifford Craig Foundation (CCF), University of Tasmania, and Waitemata District Health Board to fund participating sites for physiotherapists to provide preoperative interventions outside of current standard care and for research assistants to acquire data. JR, LA, and CH were also supported by these grants to coordinate the project at their respective sites. IKR receives a salary from the CCF to perform statistical analysis and provide study design advice for studies receiving grants from the CCF. IKR also receives information technology and library services from the University of Tasmania. Neither CCF nor the University of Tasmania have managerial authority over IKR’s work.
Figures
Comment in
-
A single preoperative physiotherapy session reduced pulmonary complications after upper abdominal surgery.Ann Intern Med. 2018 May 15;168(10):JC51. doi: 10.7326/ACPJC-2018-168-10-051. Ann Intern Med. 2018. PMID: 29800427 No abstract available.
-
Critically appraised paper: Preoperative physiotherapy education halved postoperative pulmonary complications in patients after upper abdominal surgery [commentary].J Physiother. 2018 Jul;64(3):195. doi: 10.1016/j.jphys.2018.04.004. Epub 2018 Jun 9. J Physiother. 2018. PMID: 29895418 No abstract available.
-
Critically appraised paper: Preoperative physiotherapy education halved postoperative pulmonary complications in patients after upper abdominal surgery [commentary].J Physiother. 2018 Jul;64(3):195-196. doi: 10.1016/j.jphys.2018.04.005. Epub 2018 Jun 9. J Physiother. 2018. PMID: 29895419 No abstract available.
-
Critically appraised paper: Preoperative physiotherapy education halved postoperative pulmonary complications in patients after upper abdominal surgery [commentary].J Physiother. 2018 Jul;64(3):194. doi: 10.1016/j.jphys.2018.04.006. Epub 2018 Jun 9. J Physiother. 2018. PMID: 29895420 No abstract available.
-
Critically appraised paper: Preoperative physiotherapy education halved postoperative pulmonary complications in patients after upper abdominal surgery [synopsis].J Physiother. 2018 Jul;64(3):194. doi: 10.1016/j.jphys.2018.04.008. Epub 2018 Jun 11. J Physiother. 2018. PMID: 29903596 No abstract available.
-
Boden I, Skinner EH, Browning L, et al. Preoperative physiotherapy for the prevention of respiratory complications after upper abdominal surgery: pragmatic, double blinded, multicentre randomised controlled trial. BMJ. 2018;360:j5916.AORN J. 2018 Oct;108(4):461-467. doi: 10.1002/aorn.12369. AORN J. 2018. PMID: 30265399 No abstract available.
-
Preoperative physiotherapy education prevented postoperative pulmonary complications following open upper abdominal surgery.BMJ Evid Based Med. 2019 Apr;24(2):74-75. doi: 10.1136/bmjebm-2018-110985. Epub 2018 Nov 15. BMJ Evid Based Med. 2019. PMID: 30442710 No abstract available.
References
-
- Hemmes SN, Gama de Abreu M, Pelosi P, Schultz MJ, PROVE Network Investigators for the Clinical Trial Network of the European Society of Anaesthesiology High versus low positive end-expiratory pressure during general anaesthesia for open abdominal surgery (PROVHILO trial): a multicentre randomised controlled trial. Lancet 2014;384:495-503. 10.1016/S0140-6736(14)60416-5 - DOI - PMC - PubMed
-
- Schultz MJ, Hemmes SN, Neto AS, et al. LAS VEGAS investigators Epidemiology, practice of ventilation and outcome for patients at increased risk of postoperative pulmonary complications: LAS VEGAS - an observational study in 29 countries. Eur J Anaesthesiol 2017;34:492-507. 10.1097/EJA.0000000000000646 - DOI - PMC - PubMed
-
- Neto AS, Hemmes SN, Barbas CS, et al. PROVE Network investigators Incidence of mortality and morbidity related to postoperative lung injury in patients who have undergone abdominal or thoracic surgery: a systematic review and meta-analysis. Lancet Respir Med 2014;2:1007-15. 10.1016/S2213-2600(14)70228-0 - DOI - PubMed
-
- Fernandez-Bustamante A, Frendl G, Sprung J, et al. Postoperative Pulmonary Complications, Early Mortality, and Hospital Stay Following Noncardiothoracic Surgery: A Multicenter Study by the Perioperative Research Network Investigators. JAMA Surg 2017;152:157-66. 10.1001/jamasurg.2016.4065 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical