

Comparative Cardiovascular Risk of Abatacept and Tumor Necrosis Factor Inhibitors in Patients With Rheumatoid Arthritis With and Without Diabetes Mellitus: A Multidatabase Cohort Study
- PMID: 29367417
- PMCID: PMC5850244
- DOI: 10.1161/JAHA.117.007393
Comparative Cardiovascular Risk of Abatacept and Tumor Necrosis Factor Inhibitors in Patients With Rheumatoid Arthritis With and Without Diabetes Mellitus: A Multidatabase Cohort Study
Abstract
Background: We examined the cardiovascular risk of abatacept compared with tumor necrosis factor (TNF) inhibitors in patients with rheumatoid arthritis with and without diabetes mellitus (DM).
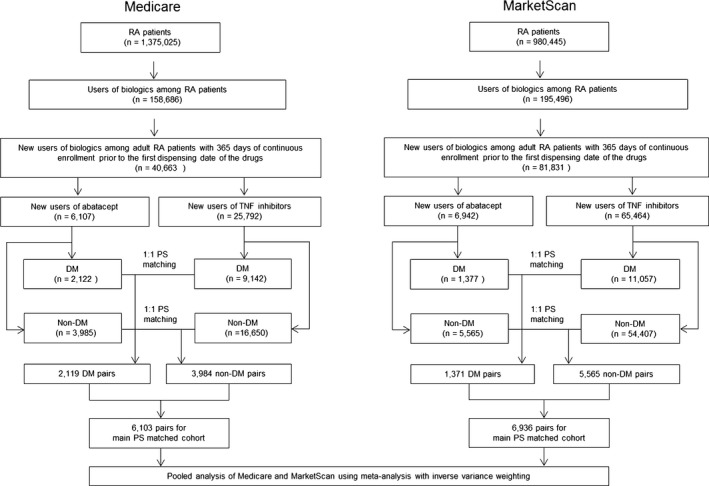
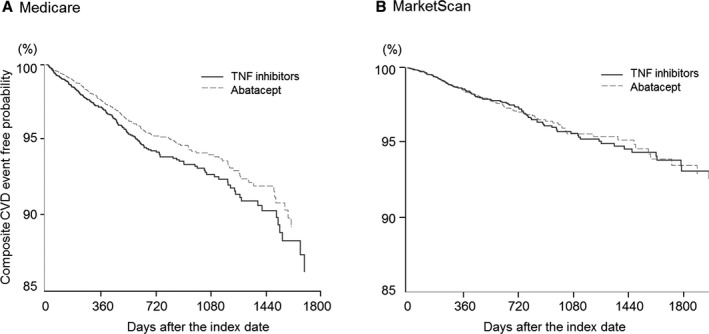
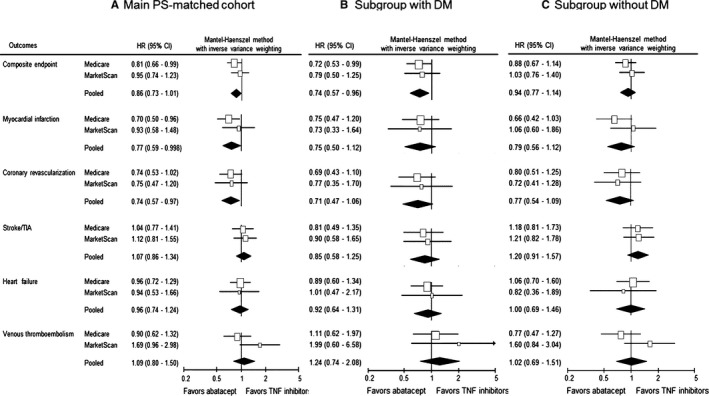
Methods and results: We conducted a cohort study of patients with rheumatoid arthritis who newly started abatacept or TNF inhibitors using claims data from Medicare and MarketScan. The primary outcome was a composite cardiovascular end point of myocardial infarction (MI), stroke/transient ischemic attack, and coronary revascularization. To account for >60 baseline characteristics, abatacept initiators were 1:1 propensity score (PS) matched to TNF initiators in each database. Cox proportional hazards models estimated hazard ratio (HR) and 95% confidence interval (CI) in the PS-matched cohort per database. A fixed-effects meta-analysis pooled database-specific HRs. We included a total of 13 039 PS-matched pairs of abatacept and TNF inhibitor initiators (6103 pairs in Medicare and 6936 pairs in MarketScan). A total of 34.7% in Medicare and 19.8% in MarketScan had baseline DM. The HR (95% CI) for the primary outcome associated with abatacept use versus TNF inhibitor was 0.81 (0.66-0.99) in Medicare and 0.95 (0.74-1.23) in MarketScan, with a pooled HR of 0.86 (95% CI, 0.73-1.01; P=0.3 for heterogeneity). The risk of the primary outcome was lower in abatacept initiators versus TNF inhibitors in the DM subgroup, with a pooled HR of 0.74 (95% CI, 0.57-0.96; P=0.7 for heterogeneity), but not in the non-DM subgroup, with a pooled HR of 0.94 (95% CI, 0.77-1.14; P=0.4 for heterogeneity).
Conclusions: In this large population-based cohort of patients with rheumatoid arthritis, abatacept use appeared to be associated with a modestly reduced cardiovascular risk when compared with TNF inhibitor use, particularly in patients with DM.
Keywords: cardiovascular disease; comparative effectiveness research; diabetes mellitus; rheumatoid arthritis; treatment.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Wolfe F, Mitchell DM, Sibley JT, Fries JF, Bloch DA, Williams CA, Spitz PW, Haga M, Kleinheksel SM, Cathey MA. The mortality of rheumatoid arthritis. Arthritis Rheum. 1994;37:481–494. - PubMed
-
- Solomon DH, Karlson EW, Rimm EB, Cannuscio CC, Mandl LA, Manson JE, Stampfer MJ, Curhan GC. Cardiovascular morbidity and mortality in women diagnosed with rheumatoid arthritis. Circulation. 2003;107:1303–1307. - PubMed
-
- Maradit‐Kremers H, Crowson CS, Nicola PJ, Ballman KV, Roger VL, Jacobsen SJ, Gabriel SE. Increased unrecognized coronary heart disease and sudden deaths in rheumatoid arthritis: a population, based cohort study. Arthritis Rheum. 2005;52:402–411. - PubMed
-
- Peters MJ, van Halm VP, Voskuyl AE, Smulders YM, Boers M, Lems WF, Visser M, Stehouwer CD, Dekker JM, Nijpels G, Heine R, Dijkmans BA, Nurmohamed MT. Does rheumatoid arthritis equal diabetes mellitus as an independent risk factor for cardiovascular disease? A prospective study. Arthritis Rheum. 2009;61:1571–1579. - PubMed
-
- del Rincón ID, Williams K, Stern MP, Freeman GL, Escalante A. High incidence of cardiovascular events in a rheumatoid arthritis cohort not explained by traditional cardiac risk factors. Arthritis Rheum. 2001;44:2737–2745. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
