

Posthemorrhagic ventricular dilatation in preterm infants: When best to intervene?
- PMID: 29367448
- PMCID: PMC5818161
- DOI: 10.1212/WNL.0000000000004984
Posthemorrhagic ventricular dilatation in preterm infants: When best to intervene?
Abstract
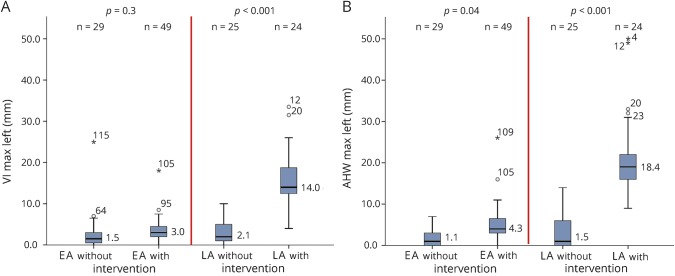
Objective: To compare neurodevelopmental outcomes of preterm infants with and without intervention for posthemorrhagic ventricular dilatation (PHVD) managed with an "early approach" (EA), based on ventricular measurements exceeding normal (ventricular index [VI] <+2 SD/anterior horn width <6 mm) with initial temporizing procedures, followed, if needed, by permanent shunt placement, and a "late approach" (LA), based on signs of increased intracranial pressure with mostly immediate permanent intervention.
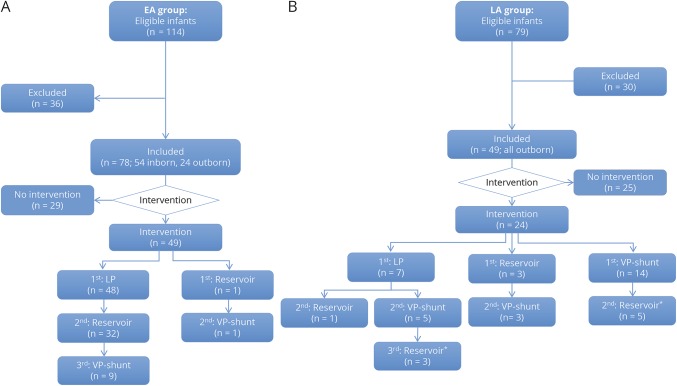
Methods: Observational cohort study of 127 preterm infants (gestation <30 weeks) with PHVD managed with EA (n = 78) or LA (n = 49). Ventricular size was measured on cranial ultrasound. Outcome was assessed at 18-24 months.
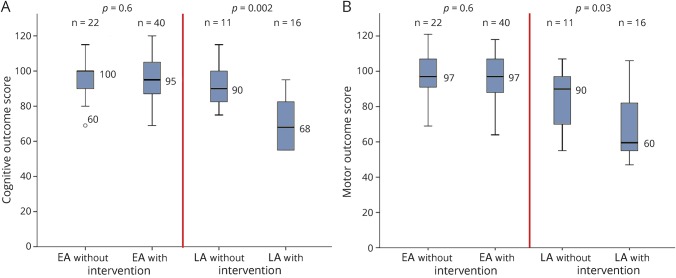
Results: Forty-nine of 78 (63%) EA and 24 of 49 (49%) LA infants received intervention. LA infants were slightly younger at birth, but did not differ from EA infants for other clinical measures. Initial intervention in the EA group occurred at younger age (29.4/33.1 week postmenstrual age; p < 0.001) with smaller ventricles (VI 2.4/14 mm >+2 SD; p < 0.01), and consisted predominantly of lumbar punctures or reservoir taps. Maximum VI in infants with/without intervention was similar in EA (3/1.5 mm >+2 SD; p = 0.3) but differed in the LA group (14/2.1 mm >+2 SD; p < 0.001). Shunt rate (20/92%; p < 0.001) and complications were lower in EA than LA group. Most EA infants had normal outcomes (>-1 SD), despite intervention. LA infants with intervention had poorer outcomes than those without (p < 0.003), with scores <-2 SD in 81%.
Conclusion: In preterm infants with PHVD, those with early intervention, even when eventually requiring a shunt, had outcomes indistinguishable from those without intervention, all being within the normal range. In contrast, in infants managed with LA, need for intervention predicted worse outcomes. Benefits of EA appear to outweigh potential risks.
Classification of evidence: This study provides Class III evidence that for preterm infants with PHVD, an EA to management results in better neurodevelopmental outcomes than a LA.
© 2018 American Academy of Neurology.
Figures
Comment in
-
Posthemorrhagic perils of prematurity.Neurology. 2018 Feb 20;90(8):351-352. doi: 10.1212/WNL.0000000000005007. Epub 2018 Jan 24. Neurology. 2018. PMID: 29367440 No abstract available.
-
Reader response: Posthemorrhagic ventricular dilatation in preterm infants: When best to intervene?Neurology. 2018 Sep 4;91(10):487. doi: 10.1212/WNL.0000000000006112. Neurology. 2018. PMID: 30177532 No abstract available.
-
Author response: Posthemorrhagic ventricular dilatation in preterm infants: When best to intervene?Neurology. 2018 Sep 4;91(10):488. doi: 10.1212/WNL.0000000000006114. Neurology. 2018. PMID: 30177533 No abstract available.
References
-
- Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weight less than 1,500 gm. J Pediatr 1978;92:529–534. - PubMed
-
- de Vries LS, Liem KD, van Dijk K, et al. ; Dutch Working Group of Neonatal Neurology. Early versus late treatment of posthaemorrhagic ventricular dilatation: results of a retrospective study from five neonatal intensive care units in the Netherlands. Acta Paediatr 2002;91:212–217. - PubMed
-
- Volpe JJ. Volpe's Neurology of the Newborn. 6th ed. Philadelphia: Elsevier; 2017;637–698.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials