

An optimised protocol for platelet-rich plasma preparation to improve its angiogenic and regenerative properties
- PMID: 29367608
- PMCID: PMC5784112
- DOI: 10.1038/s41598-018-19419-6
An optimised protocol for platelet-rich plasma preparation to improve its angiogenic and regenerative properties
Abstract
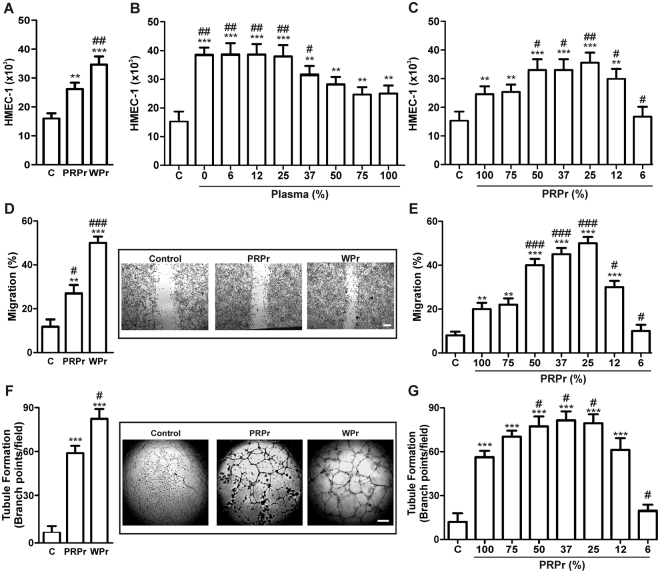
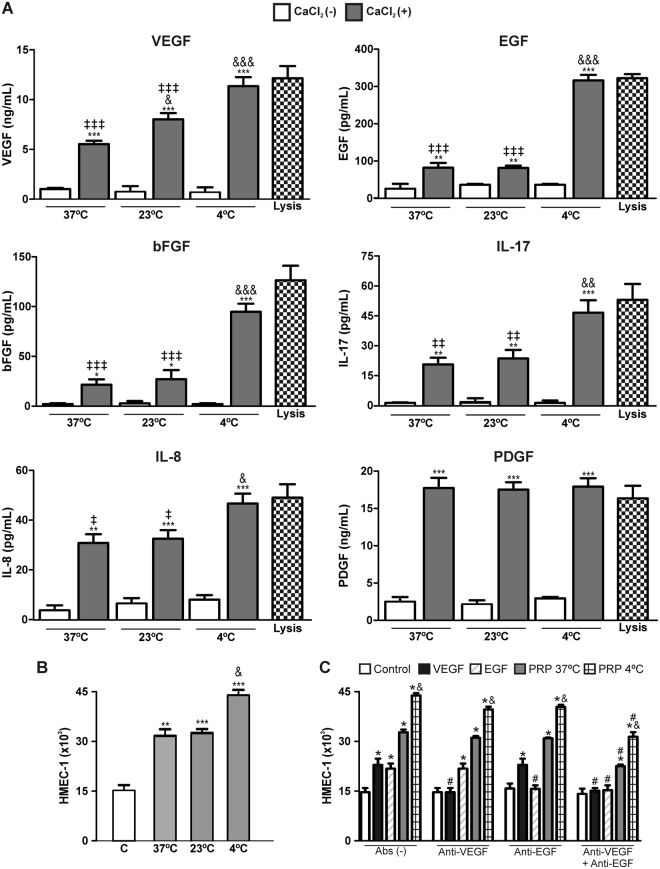
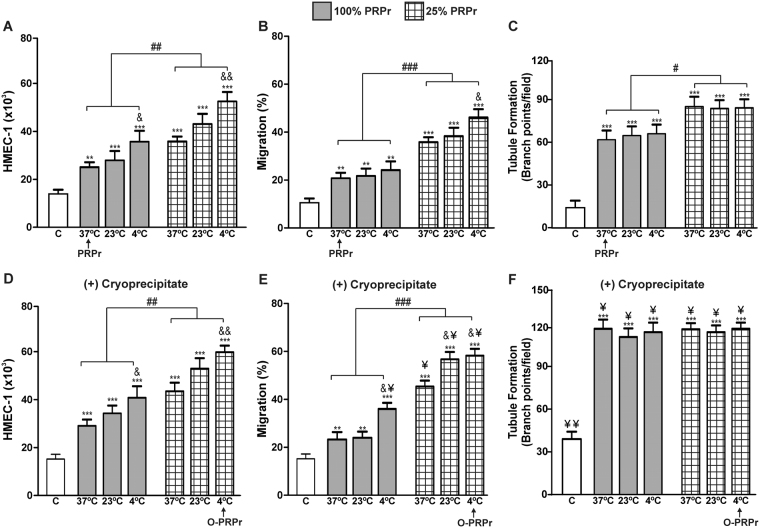
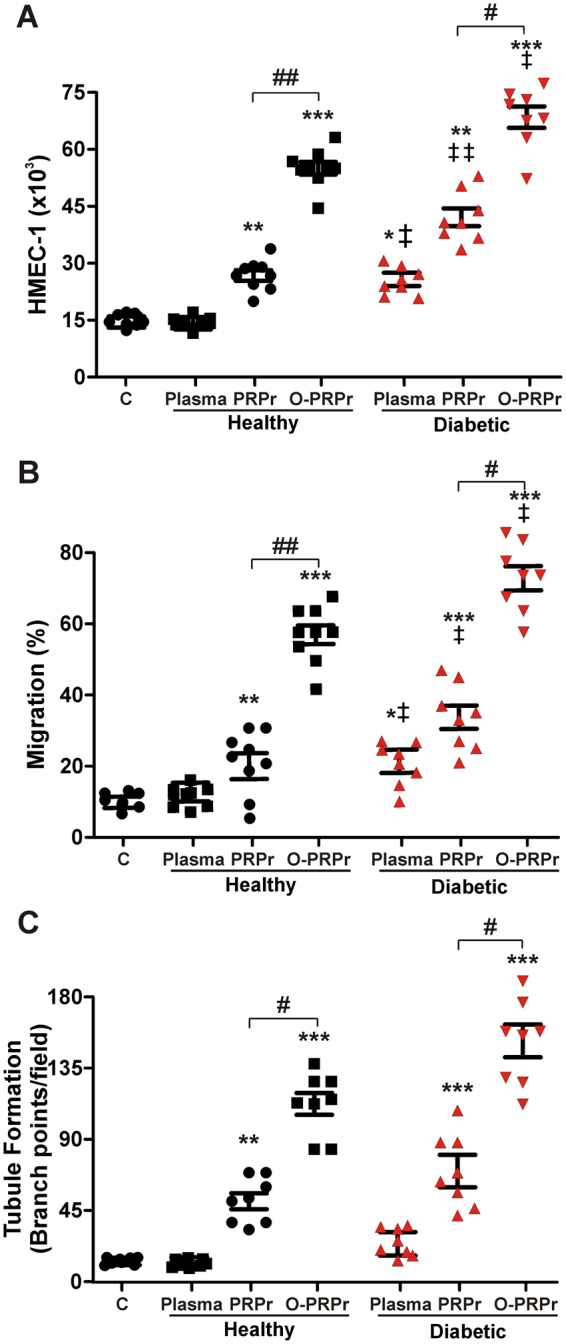
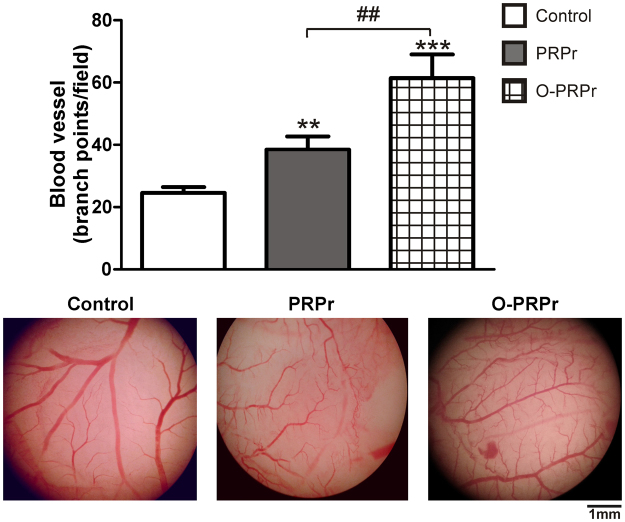
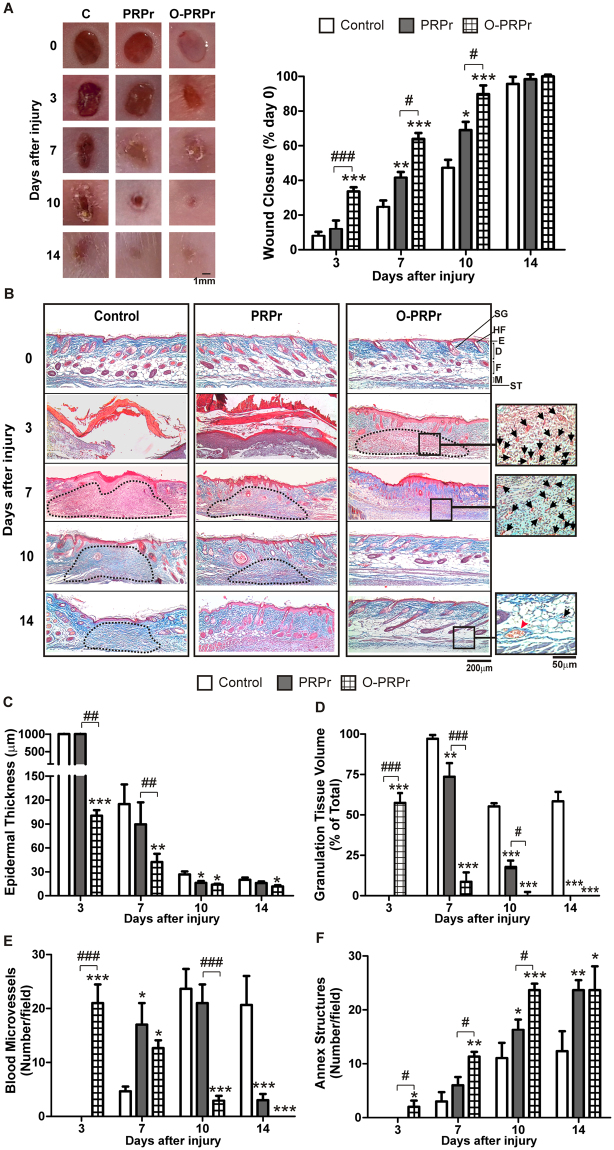
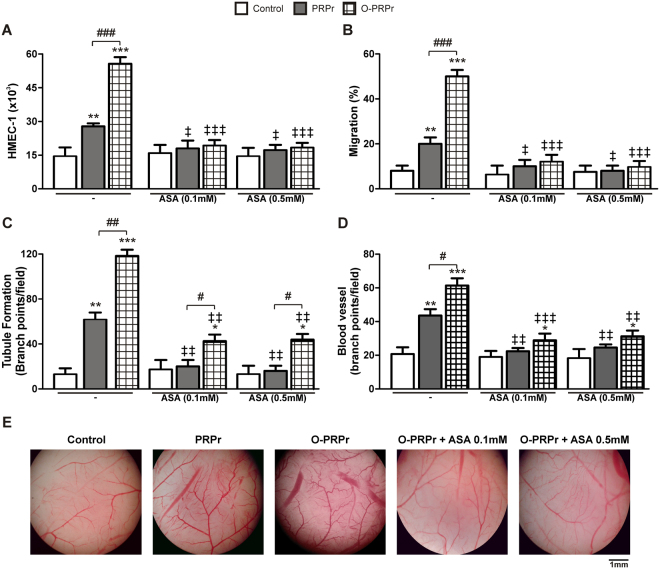
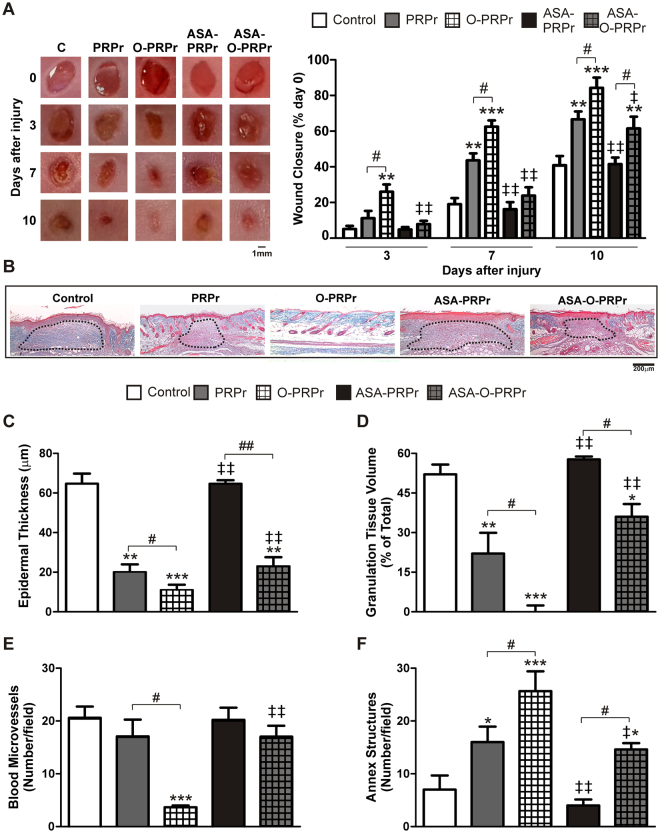
Although platelet-rich plasma (PRP) is used as a source of growth factors in regenerative medicine, its effectiveness remains controversial, partially due to the absence of PRP preparation protocols based on the regenerative role of platelets. Here, we aimed to optimise the protocol by analysing PRP angiogenic and regenerative properties. Three optimising strategies were evaluated: dilution, 4 °C pre-incubation, and plasma cryoprecipitate supplementation. Following coagulation, PRP releasates (PRPr) were used to induce angiogenesis in vitro (HMEC-1 proliferation, migration, and tubule formation) and in vivo (chorioallantoic membrane), as well as regeneration of excisional wounds on mouse skin. Washed platelet releasates induced greater angiogenesis than PRPr due to the anti-angiogenic effect of plasma, which was decreased by diluting PRPr with saline. Angiogenesis was also improved by both PRP pre-incubation at 4 °C and cryoprecipitate supplementation. A combination of optimising variables exerted an additive effect, thereby increasing the angiogenic activity of PRPr from healthy donors and diabetic patients. Optimised PRPr induced faster and more efficient mouse skin wound repair compared to that induced by non-optimised PRPr. Acetylsalicylic acid inhibited angiogenesis and tissue regeneration mediated by PRPr; this inhibition was reversed following optimisation. Our findings indicate that PRP pre-incubation at 4 °C, PRPr dilution, and cryoprecipitate supplementation improve the angiogenic and regenerative properties of PRP compared to the obtained by current methods.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
