

Central and cerebral haemodynamic changes after antihypertensive therapy in ischaemic stroke patients: A double-blind randomised trial
- PMID: 29367614
- PMCID: PMC5784025
- DOI: 10.1038/s41598-018-19998-4
Central and cerebral haemodynamic changes after antihypertensive therapy in ischaemic stroke patients: A double-blind randomised trial
Abstract
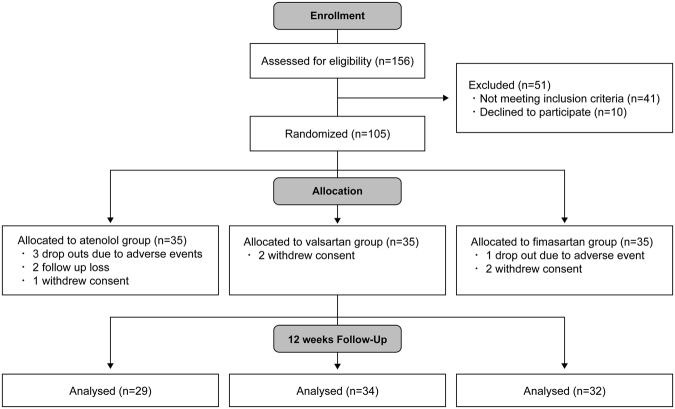
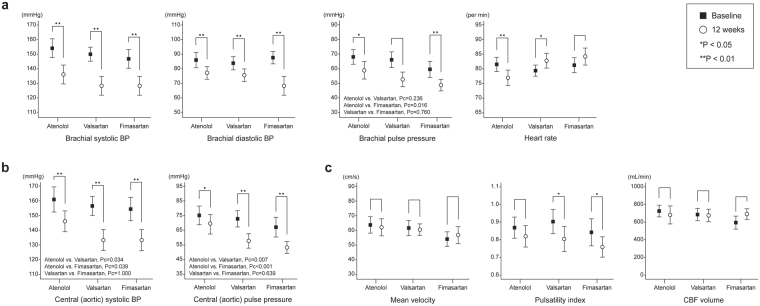
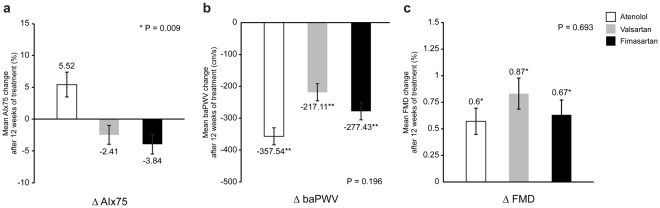
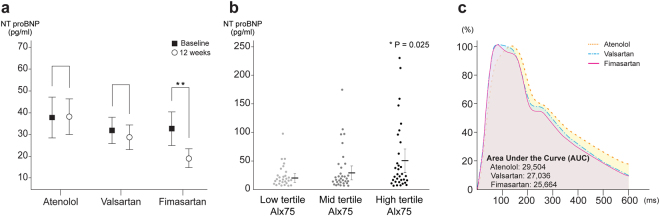
Central and cerebral haemodynamic parameters can vary under similar brachial blood pressure (BP). We aimed to investigate the effects of antihypertensive agents on central and cerebral haemodynamic parameters in hypertensive patients with ischaemic stroke. The Fimasartan, Atenolol, and Valsartan On haemodynamic paRameters (FAVOR) study was conducted in a prospective, double-blinded manner. One hundred five patients were randomly administered atenolol, valsartan, or fimasartan during 12 weeks. We measured brachial, central, cerebral haemodynamic parameters and plasma N-terminal pro-brain natriuretic peptide (NT-proBNP) levels at baseline and after 12-week. Baseline haemodynamic parameters were balanced among the three groups. Even with similar brachial BP reduction, significantly lower central systolic BP (atenolol; 146.5 ± 18.8 vs. valsartan; 133.5 ± 20.7 vs. fimasartan; 133.6 ± 19.8 mmHg, p = 0.017) and augmentation index values (89.8 ± 13.2 vs. 80.6 ± 9.2 vs. 79.2 ± 11.6%; p = 0.001) were seen in the angiotensin receptor blockers (ARBs) groups. The pulsatility index on transcranial Doppler was significantly reduced in valsartan (p = 0.002) and fimasartan group (p = 0.008). Plasma NT-proBNP level was also significantly decreased in ARB groups, especially for the fimasartan group (37.8 ± 50.6 vs. 29.2 ± 36.9 vs.19.2 ± 27.8 pg/mL; p = 0.006). These findings suggest that short-term ARB administration would be favourable for ischaemic stroke patients with hypertension, permitting effective reduction of central pressure and dampening of cerebral pulsatility.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Efficacy and safety of 30-mg fimasartan for the treatment of patients with mild to moderate hypertension: an 8-week, multicenter, randomized, double-blind, phase III clinical study.Clin Ther. 2014 Oct 1;36(10):1412-21. doi: 10.1016/j.clinthera.2014.07.004. Epub 2014 Aug 3. Clin Ther. 2014. PMID: 25092393 Clinical Trial.
-
Efficacy and tolerability of fimasartan, a new angiotensin receptor blocker, compared with losartan (50/100 mg): a 12-week, phase III, multicenter, prospective, randomized, double-blind, parallel-group, dose escalation clinical trial with an optional 12-week extension phase in adult Korean patients with mild-to-moderate hypertension.Clin Ther. 2012 Mar;34(3):552-568, 568.e1-9. doi: 10.1016/j.clinthera.2012.01.024. Epub 2012 Mar 3. Clin Ther. 2012. PMID: 22381711 Clinical Trial.
-
24-Hour blood pressure response to lower dose (30 mg) fimasartan in Korean patients with mild to moderate essential hypertension.Korean J Intern Med. 2017 Nov;32(6):1025-1036. doi: 10.3904/kjim.2016.094. Epub 2017 Oct 17. Korean J Intern Med. 2017. PMID: 29032666 Free PMC article. Clinical Trial.
-
Comparison of the Effect of Fimasartan versus Valsartan on Blood Pressure Variability in Acute Ischemic Stroke: A Double-Blind Randomized Trial.Cardiovasc Ther. 2019 Jun 2;2019:7836527. doi: 10.1155/2019/7836527. eCollection 2019. Cardiovasc Ther. 2019. PMID: 31772615 Free PMC article. Clinical Trial.
-
Efficacy of Zofenopril vs. Irbesartan in Combination with a Thiazide Diuretic in Hypertensive Patients with Multiple Risk Factors not Controlled by a Previous Monotherapy: A Review of the Double-Blind, Randomized "Z" Studies.Adv Ther. 2017 Apr;34(4):784-798. doi: 10.1007/s12325-017-0497-8. Epub 2017 Mar 4. Adv Ther. 2017. PMID: 28260186 Free PMC article. Review.
Cited by
-
Antihypertensive Treatment and Central Arterial Hemodynamics: A Meta-Analysis of Randomized Controlled Trials.Front Physiol. 2021 Nov 24;12:762586. doi: 10.3389/fphys.2021.762586. eCollection 2021. Front Physiol. 2021. PMID: 34899387 Free PMC article.
-
Circulating microparticles and central blood pressure according to antihypertensive strategy.Clinics (Sao Paulo). 2019 Nov 11;74:e1234. doi: 10.6061/clinics/2019/e1234. eCollection 2019. Clinics (Sao Paulo). 2019. PMID: 31721907 Free PMC article. Clinical Trial.
-
Two-Drug Combinations Therapy of Different Doses of Valsartan Existing Diverse Significance for Hypertensive Patients.Rev Cardiovasc Med. 2023 Jun 29;24(7):187. doi: 10.31083/j.rcm2407187. eCollection 2023 Jul. Rev Cardiovasc Med. 2023. PMID: 39077003 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
