

Variation in laparoscopic anti-reflux surgery across England: a 5-year review
- PMID: 29368285
- PMCID: PMC5988770
- DOI: 10.1007/s00464-018-6038-y
Variation in laparoscopic anti-reflux surgery across England: a 5-year review
Abstract
Background: Laparoscopic anti-reflux surgery (LARS) remains central to the management of gastro-oesophageal reflux disease but the scale and variation in provision in England is unknown. The aims of this study were firstly to examine the processes and outcomes of anti-reflux surgery in England and compare them to national guidelines and secondly to explore potential variations in practice nationally and establish peer benchmarks.
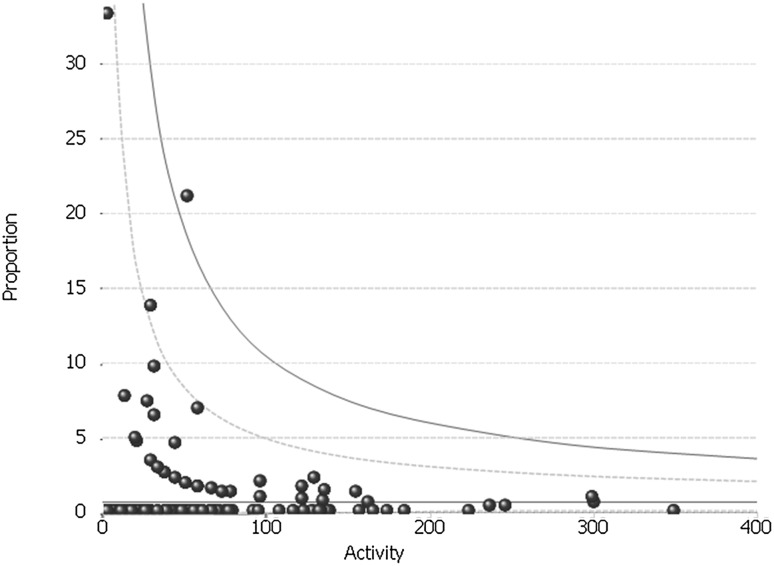
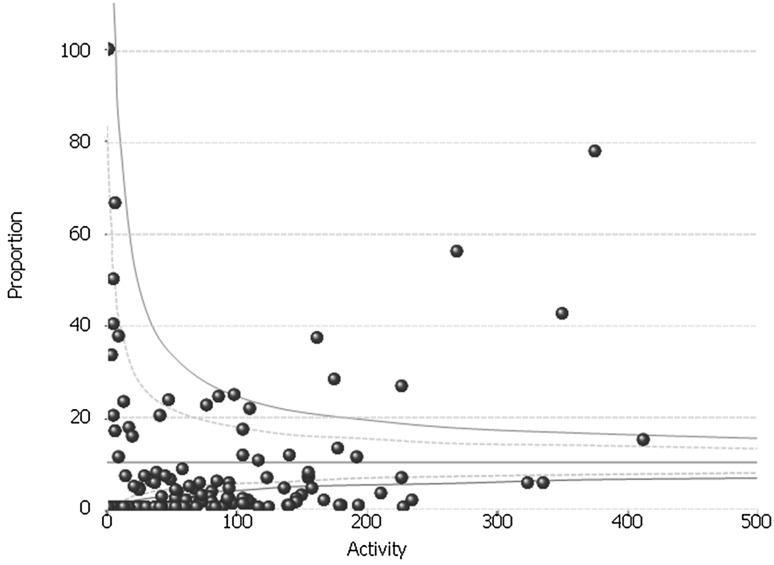
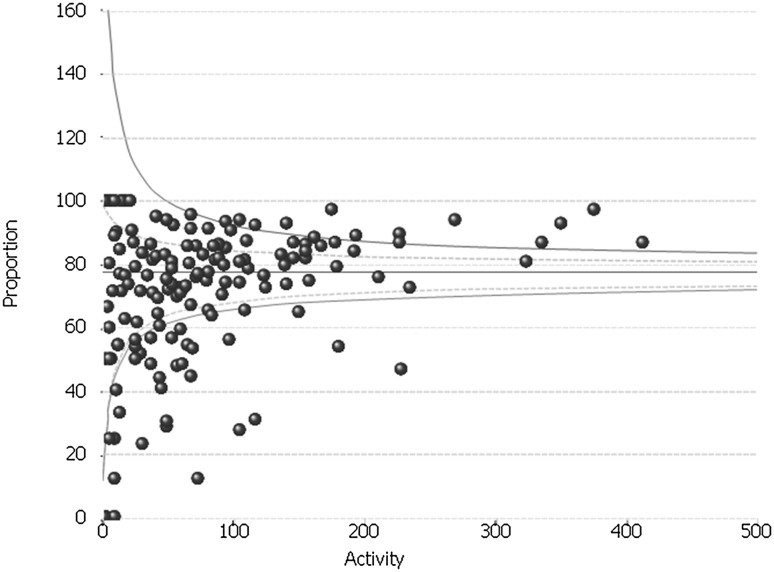
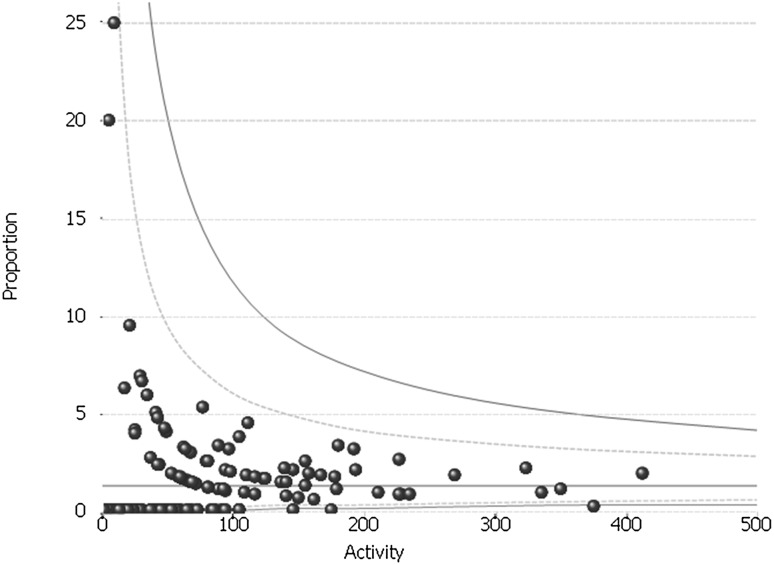
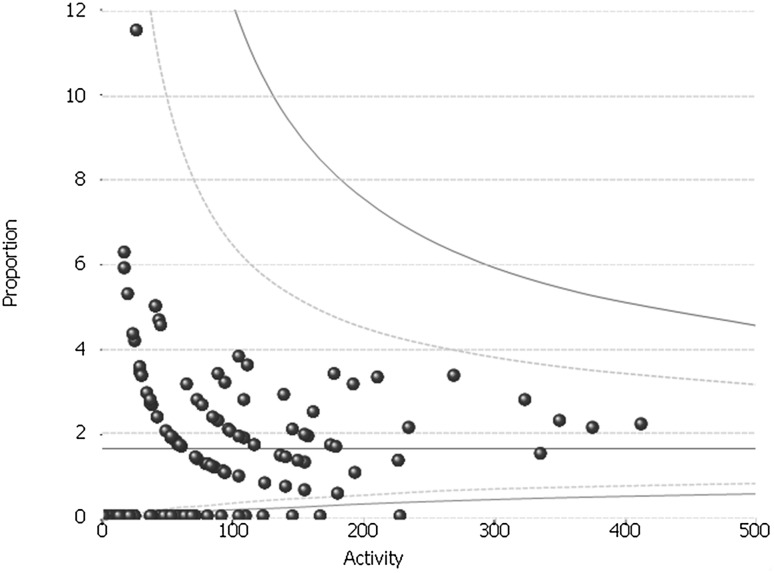
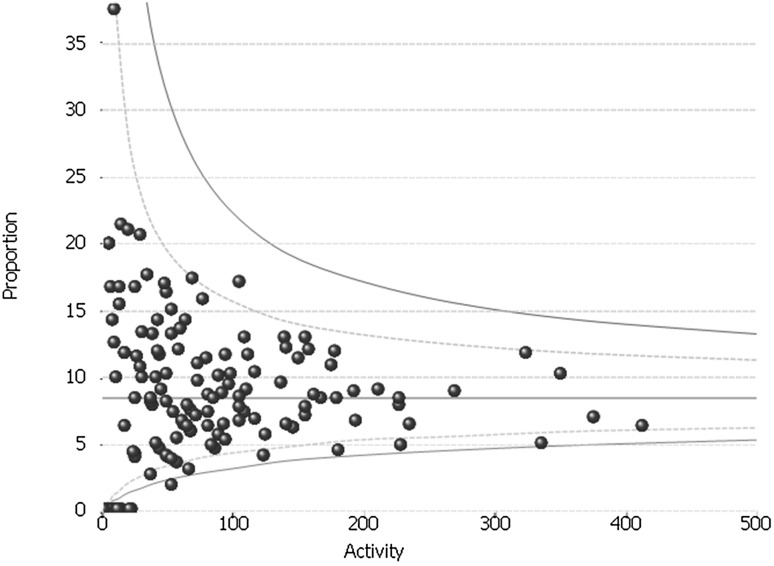
Methods: All adult patients who underwent LARSin England during the Financial years FY 2011/2012-FY 2016/2017 were identified in the Surgeon's Workload Outcomes and Research Database (SWORD), which is based on the Hospital Episode Statistics (HES) data warehouse. Outcomes included activity volume, day-case rate, short-stay rate, 2- and 30-day readmission rates and 30-day re-operation rates. Funnel plots were used to identify national variation in practice.
Results: In total, 12,086 patients underwent LARS in England during the study period. The operation rate decreased slightly over the study period from 5.2 to 4.6 per 100,000 people. Most outcomes were in line with national guidelines including the conversion rate (0.76%), 30-day re-operation rate (1.43%) and 2- and 30-day readmission rates (1.65 and 8.54%, respectively). The day-case rate was low but increased from 7.4 to 15.1% during the 5-year period. Significant variation was found, particularly in terms of hospital volume, and day-case, short-stay and conversion rates.
Conclusion: Although overall outcomes are comparable to studies from other countries, there is significant variation in anti-reflux surgery activity and outcomes in England. We recommend that units use these data to drive local quality improvement efforts.
Keywords: Anti-reflux surgery; Variation.
Conflict of interest statement
Dr. Swift is Managing Director of Methods Analytics Ltd. which undertakes paid work on behalf of a variety of organisations including the Royal College of Surgeons of England; Methods Analytics has not been paid for work on this paper. Mr. Ceney and Mr. Knight are paid employee of Methods Analytics Ltd. Their duties include performing some of the analysis included in this paper. Dr. Beckingham is Past President of the Association of Upper Gastro-Intestinal Surgeons of Great Britain and Ireland (AUGIS), past secretary of the Association of Laparoscopic Surgeons of Great Britain and Ireland and is chair of the AUGIS/Royal College of Surgeons of England Commissioning Guide for Gallstone disease. Dr. Palser, Dr. Navarro and Professor Bowrey have no conflicts of interest or financial ties to disclose.
Figures
References
-
- Wileman SM, McCann S, Grant AM, Krukowski ZH, Bruce J. Medical versus surgical management for gastro-oesophageal reflux disease (GORD) in adults. Cochrane Database Syst Rev. 2010;17(3):CD003243. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
