

Dolutegravir pharmacokinetics in pregnant and postpartum women living with HIV
- PMID: 29369162
- PMCID: PMC5854536
- DOI: 10.1097/QAD.0000000000001755
Dolutegravir pharmacokinetics in pregnant and postpartum women living with HIV
Abstract
Objective: To evaluate dolutegravir pharmacokinetics during pregnancy compared with postpartum and in infant washout samples after delivery.
Design: Ongoing, nonrandomized, open-label, parallel-group, multicenter phase-IV prospective study of antiretroviral pharmacokinetics in HIV-infected pregnant women and infants.
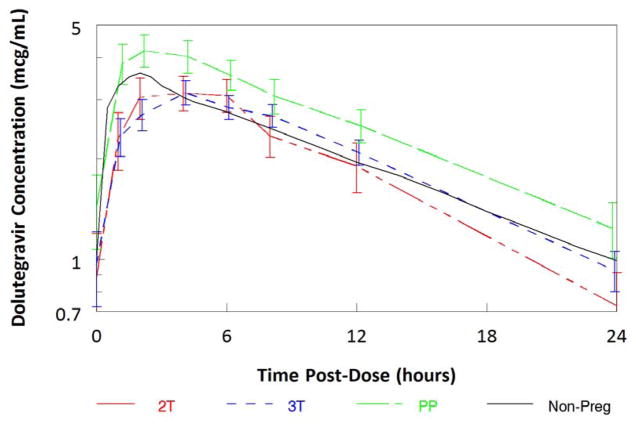
Methods: Intensive steady-state 24 h pharmacokinetic profiles after dolutegravir 50 mg once-daily were performed during the second trimester (2T), third trimester (3T) and postpartum. Maternal delivery and postnatal infant samples were collected after birth. Dolutegravir was measured by validated LC-MS/MS; quantitation limit was 0.005 μg/ml. A two-tailed Wilcoxon signed-rank test (α = 0.10) was employed for paired within-subject comparisons.
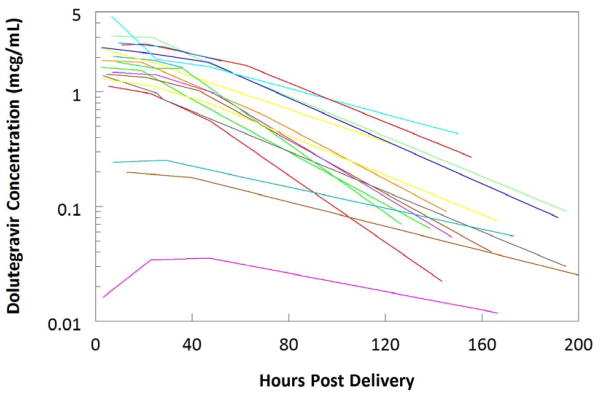
Results: Twenty-nine enrolled participants had a median age of 32 years (range 21-42). Pharmacokinetic data were available for 15 (2T), 28 (3T) and 23 (postpartum) women. Median dolutegravir AUC0-24,Cmax and C24 were 25-51% lower in the 2T and 3T compared with postpartum. The median cord blood/maternal plasma concentration ratio was 1.25 (n = 18). In 21 infants, median elimination half-life was 32.8 h after in utero exposure. Viral load at delivery was less than 50 copies/ml for 27/29 women (93%). Twenty-nine infants were HIV-negative. Renal abnormalities noted on ultrasound in two infants were deemed possibly related to dolutegravir.
Conclusion: Dolutegravir exposure is lower in pregnancy compared with postpartum in the same women on once-daily dosing. Median AUC0-24 during pregnancy was similar to, whereas trough concentrations were lower than, those seen in nonpregnant adults. Trough concentrations in pregnancy were well above dolutegravir EC90 (0.064 μg/ml). Dolutegravir readily crosses the placenta. Infant elimination is prolonged, with half-life over twice that of historical adult controls.
Conflict of interest statement
Overall support for the International Maternal Pediatric Adolescent AIDS Clinical Trials Network (IMPAACT) was provided by the National Institute of Allergy and Infectious Diseases (NIAID) of the National Institutes of Health (NIH) under Award Numbers UM1AI068632 (IMPAACT LOC), UM1AI068616 (IMPAACT SDMC) and UM1AI106716 (IMPAACT LC), with co-funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) and the National Institute of Mental Health (NIMH). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. No author conflicts were declared.
Figures
Similar articles
-
Safety and pharmacokinetics of dolutegravir in pregnant mothers with HIV infection and their neonates: A randomised trial (DolPHIN-1 study).PLoS Med. 2019 Sep 20;16(9):e1002895. doi: 10.1371/journal.pmed.1002895. eCollection 2019 Sep. PLoS Med. 2019. PMID: 31539371 Free PMC article. Clinical Trial.
-
Elvitegravir/cobicistat pharmacokinetics in pregnant and postpartum women with HIV.AIDS. 2018 Nov 13;32(17):2507-2516. doi: 10.1097/QAD.0000000000001992. AIDS. 2018. PMID: 30134297 Free PMC article. Clinical Trial.
-
Pharmacokinetics and safety of dolutegravir in children receiving rifampicin tuberculosis treatment in South Africa (ORCHID): a prospective cohort study.Lancet HIV. 2025 Apr;12(4):e273-e282. doi: 10.1016/S2352-3018(24)00312-6. Epub 2025 Feb 26. Lancet HIV. 2025. PMID: 40023169 Clinical Trial.
-
Pharmacokinetics and Safety of the Integrase Inhibitors Elvitegravir and Dolutegravir in Pregnant Women With HIV.Ann Pharmacother. 2019 Aug;53(8):833-844. doi: 10.1177/1060028019830788. Epub 2019 Feb 10. Ann Pharmacother. 2019. PMID: 30739498 Review.
-
Pharmacology of HIV integrase inhibitors.Curr Opin HIV AIDS. 2012 Sep;7(5):390-400. doi: 10.1097/COH.0b013e328356e91c. Curr Opin HIV AIDS. 2012. PMID: 22789987 Free PMC article. Review.
Cited by
-
Validation and clinical application of a novel LC-MS method for quantification of dolutegravir in breast milk.Bioanalysis. 2018 Dec;10(23):1933-1945. doi: 10.4155/bio-2018-0085. Epub 2018 Nov 19. Bioanalysis. 2018. PMID: 30450920 Free PMC article.
-
Long-acting dolutegravir formulations prevent neurodevelopmental impairments in a mouse model.Front Pharmacol. 2023 Dec 12;14:1294579. doi: 10.3389/fphar.2023.1294579. eCollection 2023. Front Pharmacol. 2023. PMID: 38149054 Free PMC article.
-
Inclusion of pregnant women in antiretroviral drug research: what is needed to move forwards?J Int AIDS Soc. 2019 Sep;22(9):e25372. doi: 10.1002/jia2.25372. J Int AIDS Soc. 2019. PMID: 31529598 Free PMC article.
-
Role of Dolutegravir/Lamivudine in the Management of Pregnant People Living with HIV-1: A Narrative Review.Infect Dis Ther. 2025 Jan;14(1):59-80. doi: 10.1007/s40121-024-01085-z. Epub 2024 Dec 9. Infect Dis Ther. 2025. PMID: 39652285 Free PMC article. Review.
-
Antiretroviral Therapy in Pregnancy: A 2023 Review of the Literature.Curr HIV/AIDS Rep. 2024 Feb;21(1):1-10. doi: 10.1007/s11904-024-00688-y. Epub 2024 Jan 26. Curr HIV/AIDS Rep. 2024. PMID: 38277098 Free PMC article. Review.
References
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of Health and Human Services; [Section accessed February 26, 2017]. Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/AdultandAdolescentGL.pdf.
-
- Panel on Antiretroviral Therapy and Medical Management of HIV-Infected Children. [Accessed February 26, 2017];Guidelines for the Use of Antiretroviral Agents in Pediatric HIV Infection. Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/pediatricguidelines.pdf. - PubMed
-
- Loebstein R, Lalkin A, Koren G. Pharmacokinetic changes during pregnancy and their clinical relevance. Clin Pharmacokinet. 1997;33:328–343. - PubMed
-
- Stek AM, Mirochnick M, Capparelli E, Best BM, Hu C, Burchett SK, et al. Reduced lopinavir exposure during pregnancy. AIDS. 2006;20:1931–1939. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
