

HIV-positive women have higher risk of human papilloma virus infection, precancerous lesions, and cervical cancer
- PMID: 29369827
- PMCID: PMC5854529
- DOI: 10.1097/QAD.0000000000001765
HIV-positive women have higher risk of human papilloma virus infection, precancerous lesions, and cervical cancer
Abstract
Objective: HIV-positive women have higher human papillomavirus (HPV) prevalence and cervical cancer incidence than HIV-negative women, partly because of HIV's modifying effect on HPV pathogenesis. We synthesized the literature on the impact of HIV on HPV natural history.
Design: Systematic review and meta-analysis.
Methods: We searched the literature for studies evaluating HPV acquisition and persistence or precancer progression by HIV status. Data on HPV natural history by HIV status, CD4 cell counts, viral load, and antiretroviral therapy (ART) were summarized using fixed effect models.
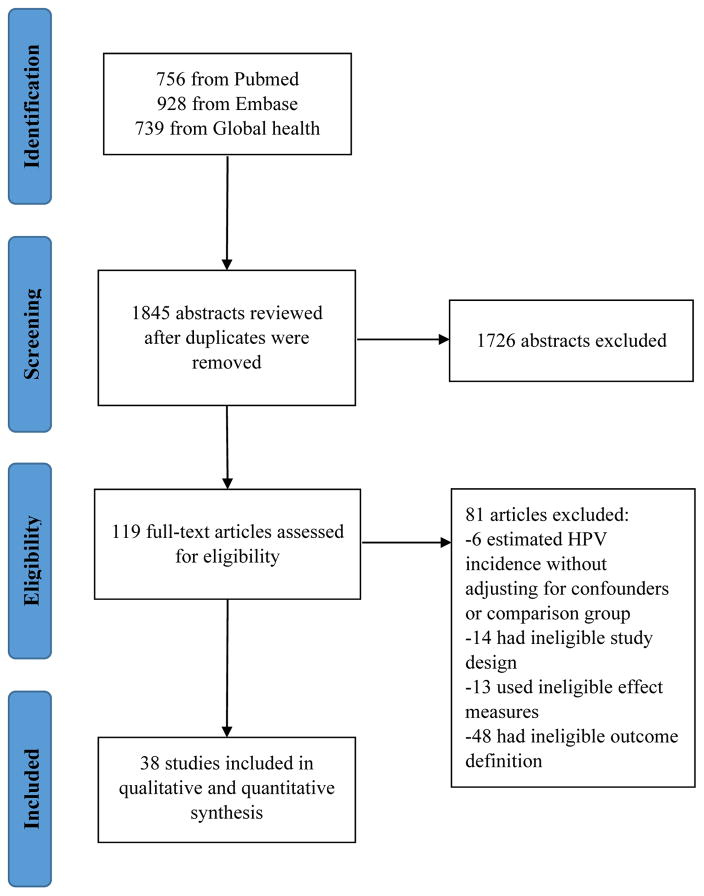
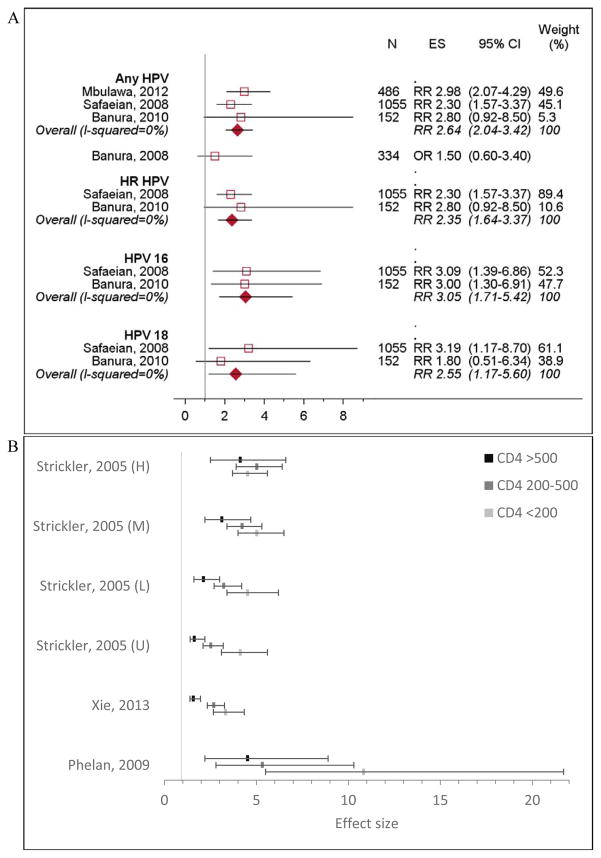
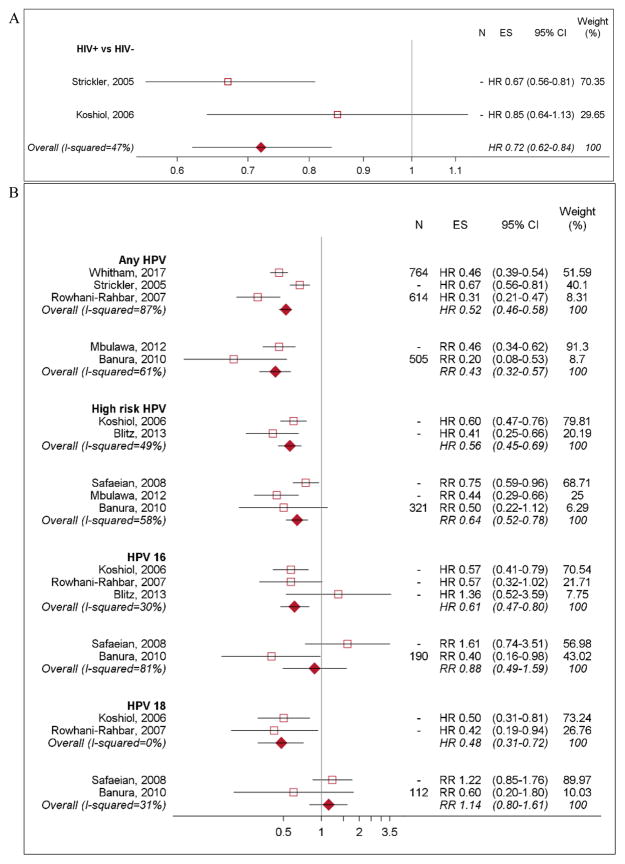
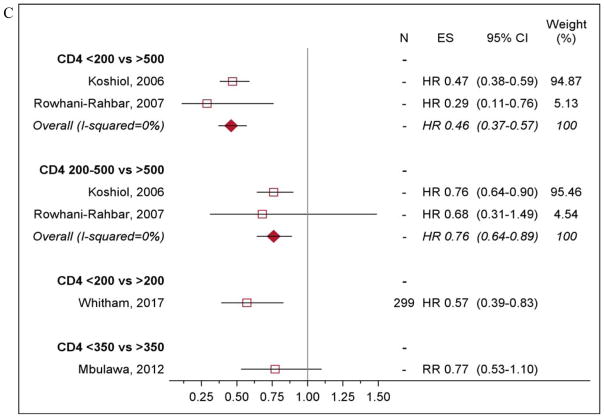
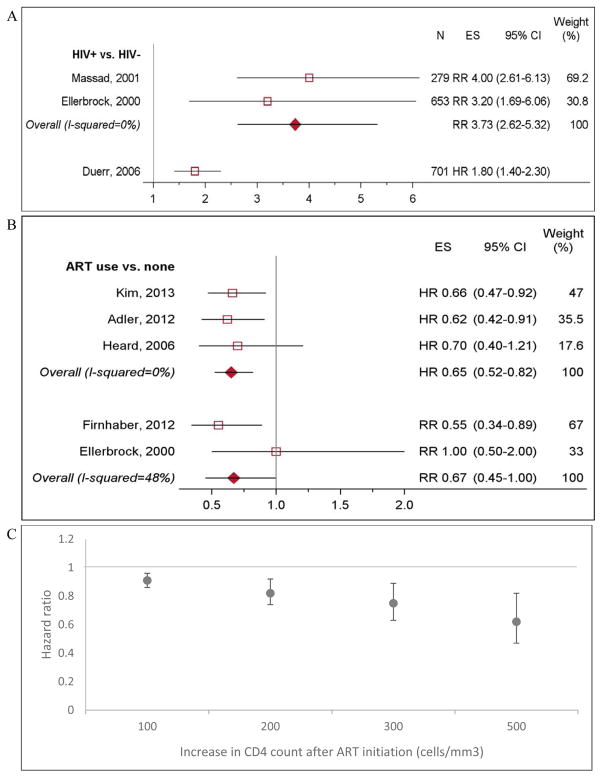
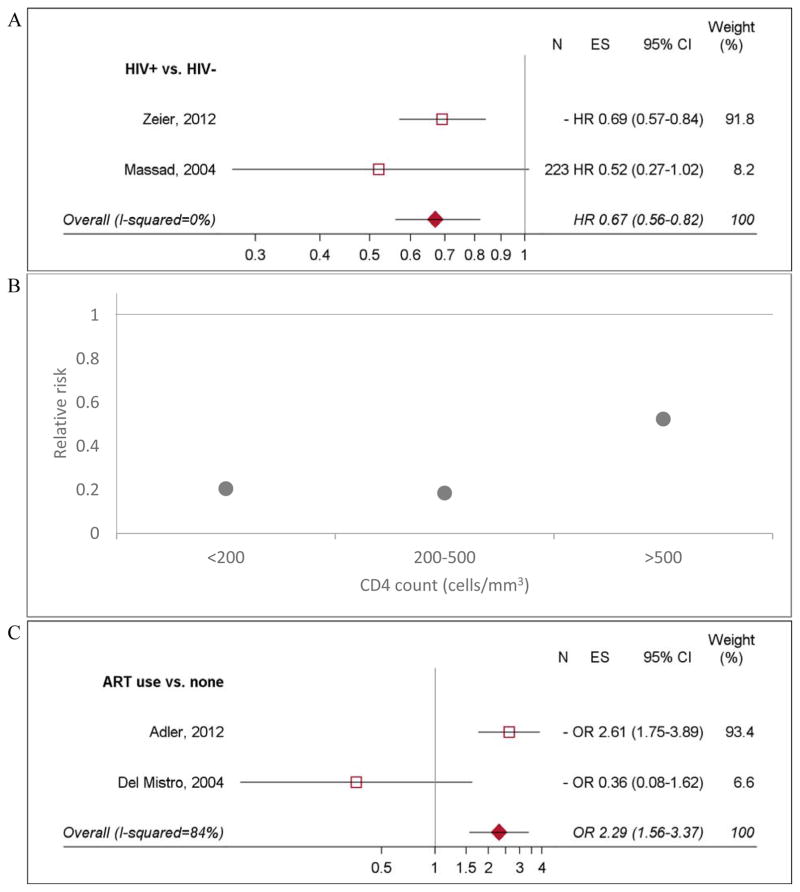
Results: Overall, 38 of 1845 abstracts identified met inclusion criteria. HIV-positive women had higher HPV acquisition [relative risk (RRpooled) 2.64, 95% confidence interval (CI) 2.04-3.42] and lower HPV clearance (hazard ratiopooled 0.72, 95% CI 0.62-0.84) than HIV-negative women. HPV acquisition was higher with declining CD4 cell count and was lower in those virally suppressed on ART. HIV was associated with higher incidence of low-grade squamous intraepithelial lesions (LSIL; RRpooled 3.73, 95% CI 2.62-5.32) and high-grade squamous intraepithelial lesions (HSIL; hazard ratiopooled 1.32, 95% CI 1.10-1.58), largely because of increased HPV persistence. ART lowered progression from normal cytology to LSIL (hazard ratiopooled 0.65, 95% CI 0.52-0.82), but not HSIL. Cervical cancer incidence was associated with HIV positivity (RR 4.1, 95% CI 2.3-6.6), but not with ART.
Conclusion: HIV-positive women have higher risk of acquiring HPV, with risk inversely associated with CD4 cell count. ART lowered HPV acquisition, increased clearance, and reduced precancer progression, likely via immune reconstitution. Although some of our results are limited by small number of studies, our study can inform screening guidelines and mathematical modeling for cervical cancer prevention.
Conflict of interest statement
The authors have no competing interests to declare.
Figures
Comment in
-
Impact of HIV on human papilloma virus-mediated cervical disease progression.AIDS. 2018 Jul 31;32(12):1715-1717. doi: 10.1097/QAD.0000000000001841. AIDS. 2018. PMID: 30001245 Free PMC article. No abstract available.
References
-
- American Cancer Society. Global cancer facts and figures. 3. Atlanta: American Cancer Society; 2015.
-
- Bruni L, Barrionuevo-Rosas L, Albero G, Serrano B, Mena M, Gómez D, et al. Human papillomavirus and related diseases in the world. Summary report. [Accessed July 6, 2017];ICO Information Centre on HPV and Cancer (HPV Information Centre) 2017
-
- Clifford GM, Franceschi S, Keiser O, Schöni-Affolter F, Lise M, Dehler S, et al. Immunodeficiency and the risk of cervical intraepithelial neoplasia 2/3 and cervical cancer: A nested case-control study in the Swiss HIV cohort study. Int J Cancer. 2016;138(7):1732–40. - PubMed
-
- Strickler HD, Burk RD, Fazzari M, Anastos K, Minkoff H, Massad LS, et al. Natural history and possible reactivation of human papillomavirus in human immunodeficiency virus-positive women. J Natl Cancer Inst. 2005;97(8):577–86. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
