

Febrile urinary-tract infection due to extended-spectrum beta-lactamase-producing Enterobacteriaceae in children: A French prospective multicenter study
- PMID: 29370234
- PMCID: PMC5784917
- DOI: 10.1371/journal.pone.0190910
Febrile urinary-tract infection due to extended-spectrum beta-lactamase-producing Enterobacteriaceae in children: A French prospective multicenter study
Abstract
Objectives: To assess the management of febrile urinary-tract infection (FUTIs) due to extended-spectrum β-lactamase-producing Enterobacteriaceae (ESBL-E) in children, the Pediatric Infectious Diseases Group of the French Pediatric Society set up an active surveillance network in pediatric centers across France in 2014.
Materials and methods: We prospectively analysed data from 2014 to 2016 for all children < 18 years old who received antibiotic treatment for FUTI due to ESBL-E in 24 pediatric centers. Baseline demographic, clinical features, microbiological data and antimicrobials prescribed were collected.
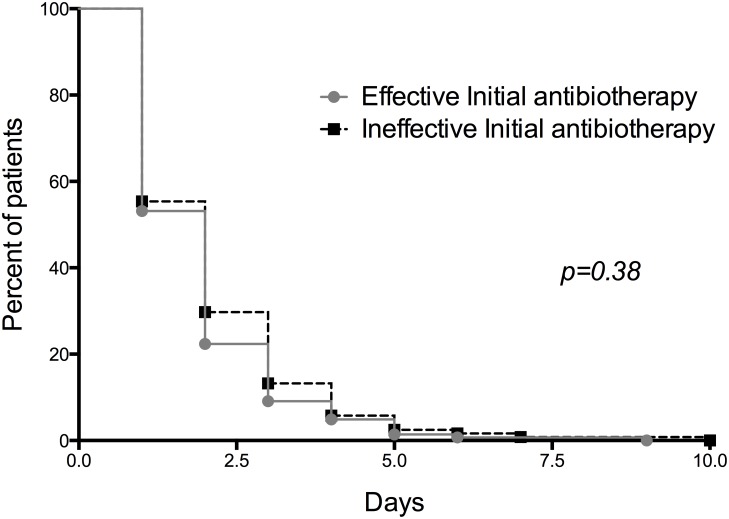
Results: 301 children were enrolled in this study. The median age was 1 year (IQR 0.02-17.9) and 44.5% were male. These infections occurred in children with history of UTIs (27.3%) and urinary malformations (32.6%). Recent antibiotic use was the main associated factor for FUTIs due to ESBL-E, followed by a previous hospitalization and travel history. Before drug susceptibility testing (DST), third-generation cephalosporins (3GC) PO/IV were the most-prescribed antibiotics (75.5%). Only 13% and 24% of children received amikacine alone for empirical or definitive therapy, respectively, whereas 88.7% of children had isolates susceptible to amikacin. In all, 23.2% of children received carbapenems in empirical and/or definitive therapy. Cotrimoxazole (24.5%), ciprofloxacin (15.6%) and non-orthodox clavulanate-cefixime combination (31.3%) were the most frequently prescribed oral options after obtaining the DST. The time to apyrexia and length of hospital stay did not differ with or without effective empirical therapy.
Conclusions: We believe that amikacin should increasingly take on a key role in the choice of definitive therapy of FUTI due to ESBL-E in children by avoiding the use of carbapenems.
Conflict of interest statement
Figures


References
-
- Montini G, Tullus K, Hewitt I. Febrile urinary tract infections in children. N Engl J Med. 2011;365: 239–250. doi: 10.1056/NEJMra1007755 - DOI - PubMed
-
- Shaikh N, Mattoo TK, Keren R, Ivanova A, Cui G, Moxey-Mims M et al. Early Antibiotic Treatment for Pediatric Febrile Urinary Tract Infection and Renal Scarring. JAMA Pediatr. 2016;170: 848–854. doi: 10.1001/jamapediatrics.2016.1181 - DOI - PubMed
-
- Hanna-Wakim RH, Ghanem ST, El Helou MW, Khafaja SA, Shaker RA, Hassan SA et al. Epidemiology and characteristics of urinary tract infections in children and adolescents. Front Cell Infect Microbiol. 2015;5: 45 doi: 10.3389/fcimb.2015.00045 - DOI - PMC - PubMed
-
- Zorc JJ, Kiddoo DA, Shaw KN. Diagnosis and management of pediatric urinary tract infections. Clin Microbiol Rev. 2005;18: 417–422. doi: 10.1128/CMR.18.2.417-422.2005 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
