

Key components of the delirium syndrome and mortality: greater impact of acute change and disorganised thinking in a prospective cohort study
- PMID: 29370764
- PMCID: PMC5785815
- DOI: 10.1186/s12877-018-0719-1
Key components of the delirium syndrome and mortality: greater impact of acute change and disorganised thinking in a prospective cohort study
Abstract
Background: Delirium increases the risk of mortality during an acute hospital admission. Full syndromal delirium (FSD) is associated with greatest risk and subsyndromal delirium (SSD) is associated with intermediate risk, compared to patients with no delirium - suggesting a dose-response relationship. It is not clear how individual diagnostic symptoms of delirium influence the association with mortality. Our objectives were to measure the prevalence of FSD and SSD, and assess the effect that FSD, SSD and individual symptoms of delirium (from the Confusion Assessment Method-short version (s-CAM)) have on mortality rates.
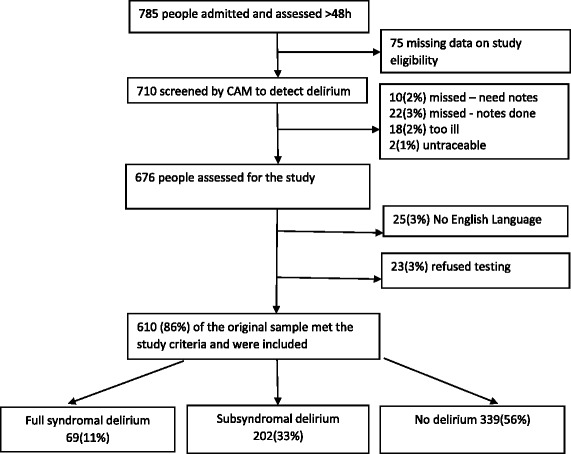
Methods: Exploratory analysis of a prospective cohort (aged ≥70 years) with acute (unplanned) medical admission (4/6/2007-4/11/2007). The outcome was mortality (data censored 6/10/2011). The principal exposures were FSD and SSD compared to no delirium (as measured by the CAM), along with individual delirium symptoms on the CAM. Cox regression was used to estimate the impact FSD and SSD and individual CAM items had on mortality.
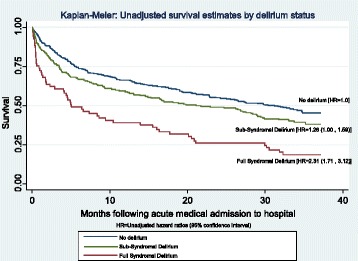
Results: The cohort (n = 610) mean age was 83 (SD 7); 59% were female. On admission, 11% had FSD and 33% had SSD. Of the key diagnostic symptoms for delirium, 17% acute onset, 19% inattention, 17% disorganised thinking and 17% altered level of consciousness. Unadjusted analysis found FSD had an increased hazard ratio (HR) of 2.31 (95% CI 1.71, 3.12), for SSD the HR was 1.26 (1.00, 1.59). Adjusted analysis remained significant for FSD (1.55 95% CI 1.10, 2.18) but nonsignificant for SSD (HR = 0.92 95% CI 0.70, 1.19). Two CAM items were significantly associated with mortality following adjustment: acute onset and disorganised thinking.
Conclusion: We observed a dose-response relationship between mortality and delirium, FSD had the greatest risk and SSD having intermediate risk. The CAM items "acute-onset" and "disorganised thinking" drove the associations observed. Clinically, this highlights the necessity of identifying individual symptoms of delirium.
Keywords: delirium; full syndromal delirium; mortality, Confusion Assessment Method, prospective cohort, acute hospital; subsyndromal delirium.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Royal Free Hospital NHS Ethics Committee (06/Q0501/31). This included the procedure for verbal consent for the original data collection, which was allowed, at the time, because this was an observational study using measures routinely collected in clinical practice. Data was de-identified before we received it and used it for this analysis.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders. 4. Washington DC: American Psychiatric Association; 1994.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
