

A randomized matched-pairs study of feasibility, acceptability, and effectiveness of systems consultation: a novel implementation strategy for adopting clinical guidelines for Opioid prescribing in primary care
- PMID: 29370813
- PMCID: PMC5784593
- DOI: 10.1186/s13012-018-0713-1
A randomized matched-pairs study of feasibility, acceptability, and effectiveness of systems consultation: a novel implementation strategy for adopting clinical guidelines for Opioid prescribing in primary care
Abstract
Background: This paper reports on the feasibility, acceptability, and effectiveness of an innovative implementation strategy named "systems consultation" aimed at improving adherence to clinical guidelines for opioid prescribing in primary care. While clinical guidelines for opioid prescribing have been developed, they have not been widely implemented, even as opioid abuse reaches epidemic levels.
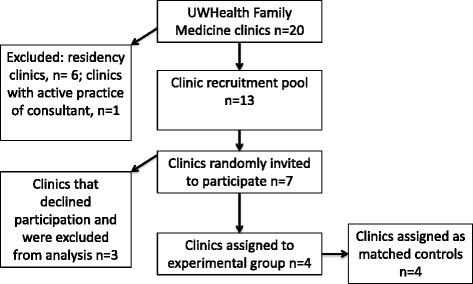
Methods: We tested a blended implementation strategy consisting of several discrete implementation strategies, including audit and feedback, academic detailing, and external facilitation. The study compares four intervention clinics to four control clinics in a randomized matched-pairs design. Each systems consultant aided clinics on implementing the guidelines during a 6-month intervention consisting of monthly site visits and teleconferences/videoconferences. The mixed-methods evaluation employs the RE-AIM (Reach, Effectiveness, Adoption, Implementation, Maintenance) framework. Quantitative outcomes are compared using time series analysis. Qualitative methods included focus groups, structured interviews, and ethnographic field techniques.
Results: Seven clinics were randomly approached to recruit four intervention clinics. Each clinic designated a project team consisting of six to eight staff members, each with at least one prescriber. Attendance at intervention meetings was 83%. More than 80% of staff respondents agreed or strongly agreed with the statements: "I am more familiar with guidelines for safe opioid prescribing" and "My clinic's workflow for opioid prescribing is easier." At 6 months, statistically significant improvements were noted in intervention clinics in the percentage of patients with mental health screens, treatment agreements, urine drug tests, and opioid-benzodiazepine co-prescribing. At 12 months, morphine-equivalent daily dose was significantly reduced in intervention clinics compared to controls. The cost to deliver the strategy was $7345 per clinic. Adaptations were required to make the strategy more acceptable for primary care. Qualitatively, intervention clinics reported that chronic pain was now treated using approaches similar to those employed for other chronic conditions, such as hypertension and diabetes.
Conclusions: The systems consultation implementation strategy demonstrated feasibility, acceptability, and effectiveness in a study involving eight primary care clinics. This multi-disciplinary strategy holds potential to mitigate the prevalence of opioid addiction and ultimately may help to improve implementation of clinical guidelines across healthcare.
Trial registration: ClinicalTrials.gov (NCT02433496). https://clinicaltrials.gov/ct2/show/NCT02433496 Registered May 5, 2015.
Keywords: Clinical practice guidelines; Evidence-based practice; Opioid prescribing; Organizational coaching; Organizational implementation strategies; Primary care.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was reviewed and approved by the University of Wisconsin – Madison’s Health Sciences Institutional Review Board, submission 2015-0280-CR002.
Consent for publication
Not applicable
Competing interests
Authors Quanbeck and Johnson have a shareholder interest in CHESS Mobile Health, a public benefit corporation that develops healthcare technology for patients struggling with addiction. This relationship is managed by the authors and the University of Wisconsin – Madison’s Conflict of Interest Committee. The other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
-
- McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristofaro A, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635–45. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
