

Single-inhaler fluticasone furoate/umeclidinium/vilanterol versus fluticasone furoate/vilanterol plus umeclidinium using two inhalers for chronic obstructive pulmonary disease: a randomized non-inferiority study
- PMID: 29370819
- PMCID: PMC5785849
- DOI: 10.1186/s12931-018-0724-0
Single-inhaler fluticasone furoate/umeclidinium/vilanterol versus fluticasone furoate/vilanterol plus umeclidinium using two inhalers for chronic obstructive pulmonary disease: a randomized non-inferiority study
Abstract
Background: Single-inhaler fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) 100/62.5/25 μg has been shown to improve lung function and health status, and reduce exacerbations, versus budesonide/formoterol in patients with chronic obstructive pulmonary disease (COPD). We evaluated the non-inferiority of single-inhaler FF/UMEC/VI versus FF/VI + UMEC using two inhalers.
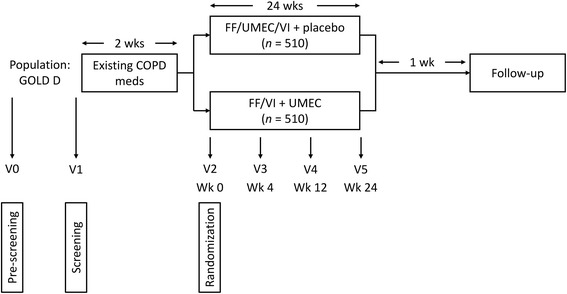
Methods: Eligible patients with COPD (aged ≥40 years; ≥1 moderate/severe exacerbation in the 12 months before screening) were randomized (1:1; stratified by the number of long-acting bronchodilators [0, 1 or 2] per day during run-in) to receive 24-week FF/UMEC/VI 100/62.5/25 μg and placebo or FF/VI 100/25 μg + UMEC 62.5 μg; all treatments/placebo were delivered using the ELLIPTA inhaler once-daily in the morning. Primary endpoint: change from baseline in trough forced expiratory volume in 1 s (FEV1) at Week 24. The non-inferiority margin for the lower 95% confidence limit was set at - 50 mL.
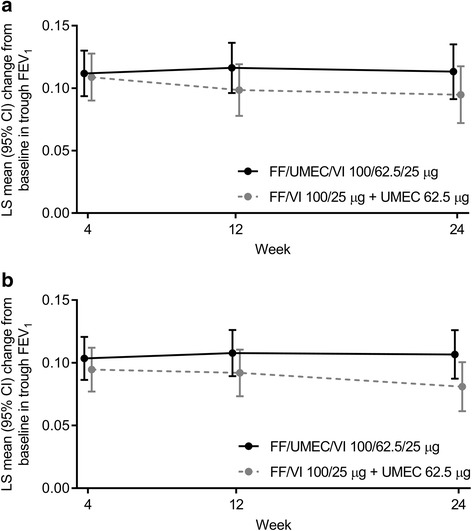
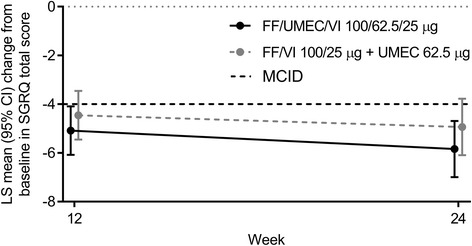
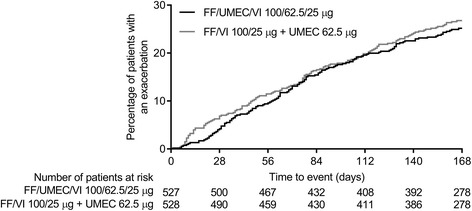
Results: A total of 1055 patients (844 [80%] of whom were enrolled on combination maintenance therapy) were randomized to receive FF/UMEC/VI (n = 527) or FF/VI + UMEC (n = 528). Mean change from baseline in trough FEV1 at Week 24 was 113 mL (95% CI 91, 135) for FF/UMEC/VI and 95 mL (95% CI 72, 117) for FF/VI + UMEC; the between-treatment difference of 18 mL (95% CI -13, 50) confirmed FF/UMEC/VI's was considered non-inferior to FF/VI + UMEC. At Week 24, the proportion of responders based on St George's Respiratory Questionnaire Total score was 50% (FF/UMEC/VI) and 51% (FF/VI + UMEC); the proportion of responders based on the Transitional Dyspnea Index focal score was similar (56% both groups). A similar proportion of patients experienced a moderate/severe exacerbation in the FF/UMEC/VI (24%) and FF/VI + UMEC (27%) groups; the hazard ratio for time to first moderate/severe exacerbation with FF/UMEC/VI versus FF/VI + UMEC was 0.87 (95% CI 0.68, 1.12). The incidence of adverse events was comparable in both groups (48%); the incidence of serious adverse events was 10% (FF/UMEC/VI) and 11% (FF/VI + UMEC).
Conclusions: Single-inhaler triple therapy (FF/UMEC/VI) is non-inferior to two inhalers (FF/VI + UMEC) on trough FEV1 change from baseline at 24 weeks. Results were similar on all other measures of efficacy, health-related quality of life, and safety.
Trial registration: GSK study CTT200812; ClinicalTrials.gov NCT02729051 (submitted 31 March 2016).
Keywords: COPD; Exacerbations; FEV1; Fluticasone furoate/umeclidinium/vilanterol; Lung function; Randomized controlled trial; Single-inhaler triple therapy.
Conflict of interest statement
Ethics approval and consent to participate
The protocol was approved by applicable institutional review boards/ethics committees at each participating site, and was conducted in accordance with applicable regulatory requirements, ICH Good Clinical Practice guidelines, and the guiding principles of the Declaration of Helsinki. All patients provided written, informed consent prior to enrollment.
Consent for publication
Not applicable.
Competing interests
RB, NB, ASI, C-QZ, and DAL are employees of GSK and hold stocks/shares in the company. ASI is also an unpaid faculty member at McMaster University, Canada. PRB has no conflicts of interest to disclose.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease . Global strategy for the diagnosis, management and prevention of COPD. 2017.
-
- Aaron SD, Vandemheen KL, Fergusson D, Maltais F, Bourbeau J, Goldstein R, et al. Tiotropium in combination with placebo, salmeterol, or fluticasone–salmeterol for treatment of chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med. 2007;146:545–555. doi: 10.7326/0003-4819-146-8-200704170-00152. - DOI - PubMed
-
- Welte T, Miravitlles M, Hernandez P, Eriksson G, Peterson S, Polanowski T, et al. Efficacy and tolerability of budesonide/formoterol added to tiotropium in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2009;180:741–750. doi: 10.1164/rccm.200904-0492OC. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
