

The Zika Contraception Access Network: a feasibility programme to increase access to contraception in Puerto Rico during the 2016-17 Zika virus outbreak
- PMID: 29371100
- PMCID: PMC5846878
- DOI: 10.1016/S2468-2667(18)30001-X
The Zika Contraception Access Network: a feasibility programme to increase access to contraception in Puerto Rico during the 2016-17 Zika virus outbreak
Abstract
Background: Prevention of unintended pregnancy is a primary strategy to reduce adverse pregnancy and birth outcomes related to Zika virus infection. The Zika Contraception Access Network (Z-CAN) aimed to build a network of health-care providers offering client-centred contraceptive counselling and the full range of reversible contraception at no cost to women in Puerto Rico who chose to prevent pregnancy during the 2016-17 Zika virus outbreak. Here, we describe the Z-CAN programme design, implementation activities, and baseline characteristics of the first 21 124 participants.
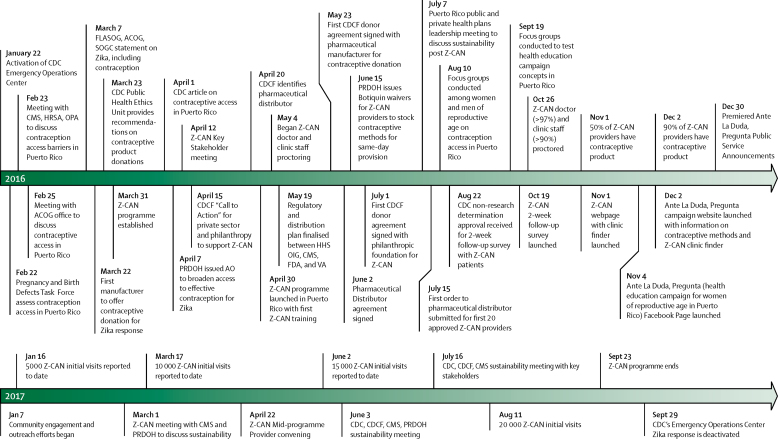
Methods: Z-CAN was developed by establishing partnerships between federal agencies, territorial health agencies, private corporations, and domestic philanthropic and non-profit organisations in the continental USA and Puerto Rico. Private donations to the National Foundation for the Centers for Disease Control and Prevention (CDCF) secured a supply of reversible contraceptive methods (including long-acting reversible contraception), made available to non-sterilised women of reproductive age at no cost through provider reimbursements and infrastructure supported by the CDCF. To build capacity in contraception service provision, doctors and clinic staff from all public health regions and nearly all municipalities in Puerto Rico were recruited into the programme. All providers completed 1 day of comprehensive training in contraception knowledge, counselling, and initiation and management, including the insertion and removal of long-acting reversible contraceptives (LARCs). Z-CAN was announced through health-care providers, word of mouth, and a health education campaign. Descriptive characteristics of programme providers and participants were recorded, and we estimated the factors associated with choosing and receiving a LARC method. As part of a Z-CAN programme monitoring plan, participants were invited to complete a patient satisfaction survey about whether they had obtained free, same-day access to their chosen contraceptive method after receiving comprehensive counselling, their perception of the quality of care they had received, and their satisfaction with their chosen method and services.
Findings: Between May 4, 2016, and Aug 15, 2017, 153 providers in the Z-CAN programme provided services to 21 124 women. 20 110 (95%) women received same-day provision of a reversible contraceptive method. Whereas only 767 (4%) women had used a LARC method before Z-CAN, 14 259 (68%) chose and received a LARC method at their initial visit. Of the women who received a LARC method, 10 808 (76%) women had used no method or a least effective method of contraception (ie, condoms or withdrawal) before their Z-CAN visit. Of the 3489 women who participated in a patient satisfaction survey, 3068 (93%) of 3294 women were very satisfied with the services received, and 3216 (93%) of 3478 women reported receiving the method that they were most interested in after receiving counselling. 2382 (78%) of 3040 women rated their care as excellent or very good.
Interpretation: Z-CAN was designed as a short-term response for rapid implementation of reversible contraceptive services in a complex emergency setting in Puerto Rico and has served more than 21 000 women. This model could be replicated or adapted as part of future emergency preparedness and response efforts.
Funding: National Foundation for the Centers for Disease Control and Prevention.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures

Comment in
-
Z-CAN: prevention of unintended pregnancy in an emergency setting.Lancet Public Health. 2018 Feb;3(2):e59-e60. doi: 10.1016/S2468-2667(18)30005-7. Epub 2018 Jan 19. Lancet Public Health. 2018. PMID: 29371101 No abstract available.
Similar articles
-
Final Program Data and Factors Associated With Long-Acting Reversible Contraception Removal: The Zika Contraception Access Network.Obstet Gynecol. 2020 May;135(5):1095-1103. doi: 10.1097/AOG.0000000000003835. Obstet Gynecol. 2020. PMID: 32282596 Free PMC article.
-
The Role of Public-Private Partnerships to Increase Access to Contraception in an Emergency Response Setting: The Zika Contraception Access Network Program.J Womens Health (Larchmt). 2020 Nov;29(11):1372-1380. doi: 10.1089/jwh.2020.8813. J Womens Health (Larchmt). 2020. PMID: 33196331 Free PMC article.
-
Program Fidelity and Patient Satisfaction among Women Served by the Zika Contraception Access Network Program in Puerto Rico.Womens Health Issues. 2020 Jul-Aug;30(4):268-276. doi: 10.1016/j.whi.2020.03.007. Epub 2020 May 4. Womens Health Issues. 2020. PMID: 32376188 Free PMC article.
-
Canadian Contraception Consensus (Part 1 of 4).J Obstet Gynaecol Can. 2015 Oct;37(10):936-42. doi: 10.1016/s1701-2163(16)30033-0. J Obstet Gynaecol Can. 2015. PMID: 26606712 English, French.
-
Understanding barriers to using long-acting reversible contraceptives (LARCs) in primary care: a qualitative evidence synthesis.BMJ Sex Reprod Health. 2023 Oct;49(4):282-292. doi: 10.1136/bmjsrh-2022-201560. Epub 2023 Feb 21. BMJ Sex Reprod Health. 2023. PMID: 36810206 Review.
Cited by
-
Response strategies for promoting gender equality in public health emergencies: a rapid scoping review.BMJ Open. 2021 Aug 12;11(8):e048292. doi: 10.1136/bmjopen-2020-048292. BMJ Open. 2021. PMID: 34385251 Free PMC article.
-
Sexual and reproductive health (SRH): a key issue in the emergency response to the coronavirus disease (COVID- 19) outbreak.Reprod Health. 2020 Apr 23;17(1):59. doi: 10.1186/s12978-020-0900-9. Reprod Health. 2020. PMID: 32326943 Free PMC article.
-
Final Program Data and Factors Associated With Long-Acting Reversible Contraception Removal: The Zika Contraception Access Network.Obstet Gynecol. 2020 May;135(5):1095-1103. doi: 10.1097/AOG.0000000000003835. Obstet Gynecol. 2020. PMID: 32282596 Free PMC article.
-
Perceptions of the Zika Virus, Contraceptive Access, and Motivation to Participate in the Zika Contraception Access Network Program: Qualitative Analysis of Focusgroup Discussions with Puerto Rican Women.P R Health Sci J. 2024 Mar;43(1):46-53. P R Health Sci J. 2024. PMID: 38512761 Free PMC article.
-
Connecting the Dots: Public Health, Clinical, and Community Connections to Improve Contraception Access.Am J Public Health. 2022 Jun;112(S5):S508-S510. doi: 10.2105/AJPH.2022.306924. Am J Public Health. 2022. PMID: 35767787 Free PMC article. No abstract available.
References
-
- Boulet SL, D'Angelo DV, Morrow B. Contraceptive use among nonpregnant and postpartum women at risk for unintended pregnancy, and female high school students, in the context of Zika preparedness—United States, 2011–2013 and 2015. MMWR Morb Mortal Wkly Rep. 2016;65:780–787. - PubMed
-
- Oussayef NL, Pillai SK, Honein MA. Zika virus—10 public health achievements in 2016 and future priorities. MMWR Morb Mortal Wkly Rep. 2016;65:1482–1488. - PubMed
-
- Lozier M, Adams L, Febo MF. Incidence of Zika virus disease by age and sex—Puerto Rico, November 1, 2015–October 20, 2016. MMWR Morb Mortal Wkly Rep. 2016;65:1219–1223. - PubMed
-
- Tepper NK, Goldberg HI, Bernal MI. Estimating contraceptive needs and increasing access to contraception in response to the Zika virus disease outbreak—Puerto Rico, 2016. MMWR Morb Mortal Wkly Rep. 2016;65:311–314. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
