

A Biomechanical Assessment of Biceps Femoris Repair Techniques
- PMID: 29372167
- PMCID: PMC5774730
- DOI: 10.1177/2325967117748891
A Biomechanical Assessment of Biceps Femoris Repair Techniques
Abstract
Background: Knee injuries encountered in clinical practice can involve avulsions of the biceps femoris from the fibula and proximal tibia. Advances in tendon repair methods now allow for repairs with increased surface areas using modern suture anchor techniques. Despite descriptions of repair techniques, there are no biomechanical studies on the biceps femoris for comparison.
Purpose/hypothesis: The objective of this controlled laboratory study was to determine the failure load of the native biceps femoris distal insertion and to evaluate modern repair techniques. Our hypothesis was 2-fold: (1) Suture repairs to the tibia and fibula would perform better on tensile testing than repairs to the fibula alone, and (2) complex bridge repairs, similar to those frequently used in rotator cuff surgery, would perform better on tensile testing than simple repairs.
Study design: Controlled laboratory study.
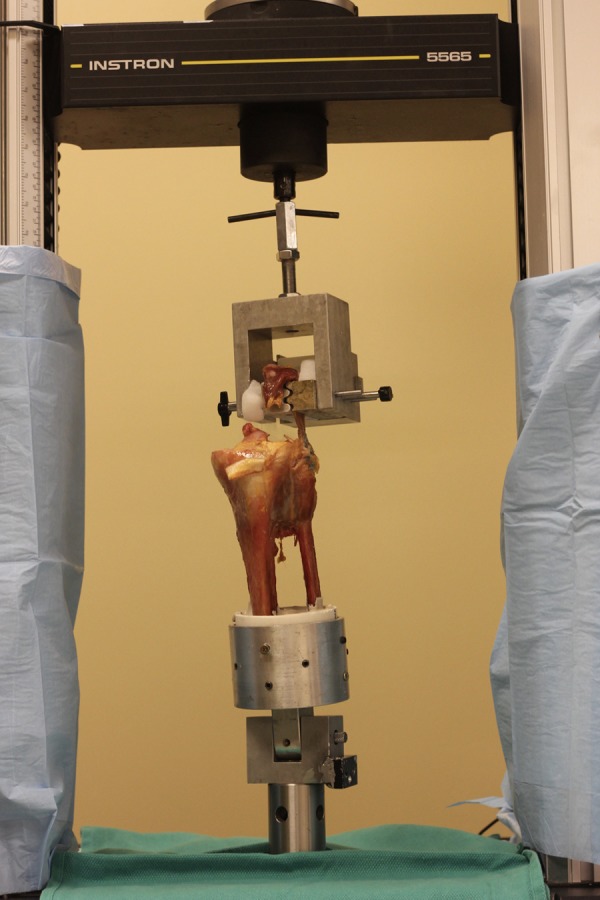
Methods: A total of 40 paired, fresh-frozen cadaveric specimens were dissected, identifying the biceps femoris and its insertion on the proximal tibia and fibula. The native biceps femoris footprint was left intact in 8 specimens and tested to failure on a uniaxial materials testing machine evaluating tensile properties, while in the other 32 specimens, the biceps femoris insertion was dissected using a No. 15 scalpel blade, underwent repair, and was then tested to failure on a uniaxial materials testing machine evaluating tensile properties. Four repair constructs were evaluated, with 8 specimens allocated for each: construct 1 involved a simple repair (ie, passing suture through tissue in a running Krackow fashion and tying at the anchor site) to the fibula with 2 suture anchors, construct 2 involved a simple repair to the fibula and tibia with 3 suture anchors, construct 3 was a fibular repair with a tibial suture bridge involving the fibula and tibia and 3 suture anchors, construct 4 involved a transosseous repair through the fibula and 1 suture anchor on the tibia. Analysis of variance was used to evaluate for significance of the mean failure load and stiffness between groups.
Results: The mean (±95% CI) failure loads were the following: native biceps femoris, 1280 ± 247.0 N; simple fibular repair, 173 ± 84.6 N; simple fibular and tibial repair, 176 ± 48.1 N; fibular repair with tibial suture bridge, 191 ± 78.5 N; and transosseous repair, 327 ± 66.3 N. The mean stiffness values were the following: native, 46 ± 13.0 N/mm; simple fibular repair, 16 ± 5.1 N/mm; simple fibular and tibial repair, 14 ± 5.4 N/mm; fibular repair with tibial suture bridge, 13 ± 2.8 N/mm; and transosseous repair, 15 ± 2.5 N/mm. Interconstruct comparison of failure loads revealed no statistical difference between constructs utilizing anchors alone. The transosseous repair showed a significant difference for the failure load when compared with each anchor repair construct (P = .02, .02, and .04 for constructs 1, 2, and 3, respectively). Interconstruct comparison of stiffness revealed no statistical difference between all constructs (P > .86). None of the repair techniques re-created the failure load or stiffness of the native biceps femoris tendon (P = .02).
Conclusion: In this biomechanical study, no difference was found between the mean failure loads of different biceps femoris repair constructs involving suture anchors alone and No. 2 braided polyester and ultra-high-molecular-weight polyethylene suture. A technique involving transosseous fibular tunnels and 2-mm suture tape illustrated a greater mean failure load than repairs relying on suture anchors for fixation.
Clinical relevance: Understanding the tensile performance of biceps femoris repair constructs aids clinicians with preoperative and intraoperative decisions. Current biceps femoris repair techniques do not approximate the native strength of the tendon. A transosseous style of repair offers the highest failure load.
Keywords: biceps femoris; failure load; posterolateral corner; repair.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: Arthrex provided financial support for the acquisition of cadaveric specimens and material support with suture anchors. A.W.A. is a paid speaker for and receives research funding from Arthrex and Smith & Nephew.
Figures





References
-
- Alioto RJ, Browne JE, Barnthouse CD, Scott AR. Complete rupture of the distal semimembranosus complex in a professional athlete. Clin Orthop Relat Res. 1997;336:162–165. - PubMed
-
- Brinkman J-M, Schwering P, Blankevoort L, Koolos J, Luites J, Wymenga A. The insertion geometry of the posterolateral corner of the knee. J Bone Joint Surg Br. 2005;87(10):1364–1368. - PubMed
-
- David A, Buchholz J, Muhr G. Tear of the biceps femoris tendon. Arch Orthop Trauma Surg. 1994;113(6):351–352. - PubMed
-
- Fortems Y, Victor J, Dauwe D, Fabry G. Isolated complete rupture of biceps femoris tendon. Injury. 1995;26(4):275–276. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
