

Non-pharmacological interventions for treating chronic prostatitis/chronic pelvic pain syndrome
- PMID: 29372565
- PMCID: PMC6491290
- DOI: 10.1002/14651858.CD012551.pub2
Non-pharmacological interventions for treating chronic prostatitis/chronic pelvic pain syndrome
Update in
-
Non-pharmacological interventions for treating chronic prostatitis/chronic pelvic pain syndrome.Cochrane Database Syst Rev. 2018 May 12;5(5):CD012551. doi: 10.1002/14651858.CD012551.pub3. Cochrane Database Syst Rev. 2018. PMID: 29757454 Free PMC article.
Abstract
Background: Chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS) is a common disorder in which the two main clinical features are pelvic pain and lower urinary tract symptoms. There are currently many approaches for its management, using both pharmacological and non-pharmacological interventions. The National Institute of Health - Chronic Prostatitis Symptom Index (NIH-CPSI) score is a validated measure commonly used to measure CP/CPPS symptoms.
Objectives: To assess the effects of non-pharmacological therapies for chronic prostatitis/chronic pelvic pain syndrome (CP/CPPS).
Search methods: We performed a comprehensive search using multiple databases, trial registries, grey literature and conference proceedings with no restrictions on the language of publication or publication status. The date of the latest search of all databases was August 2017.
Selection criteria: We included randomised controlled trials. Inclusion criteria were men with a diagnosis of CP/CPPS. We included all available non-pharmacological interventions.
Data collection and analysis: Two review authors independently classified studies and abstracted data from the included studies, performed statistical analyses and rated quality of evidence (QoE) according to the GRADE methods.
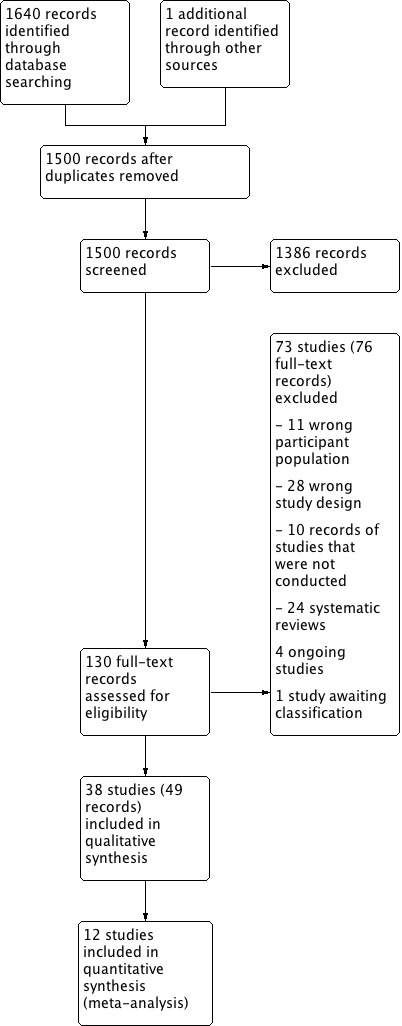
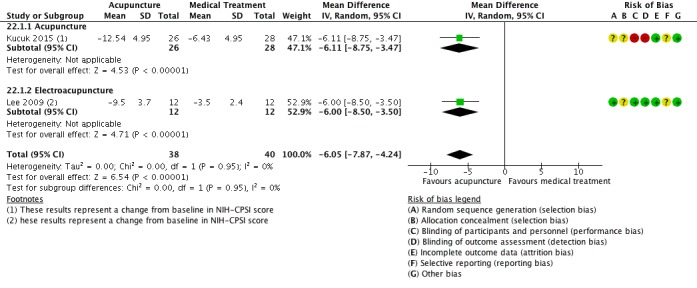
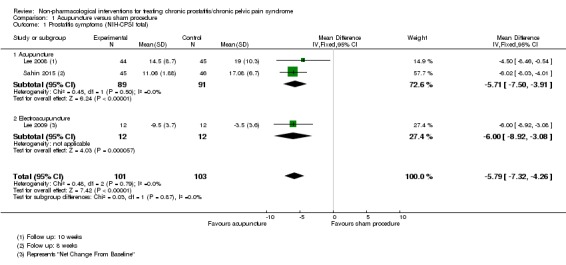
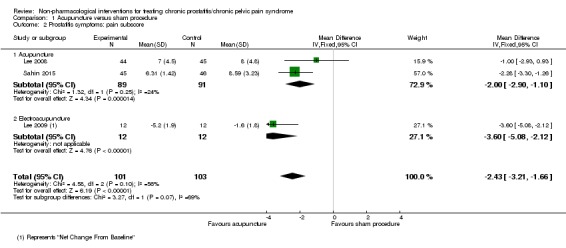
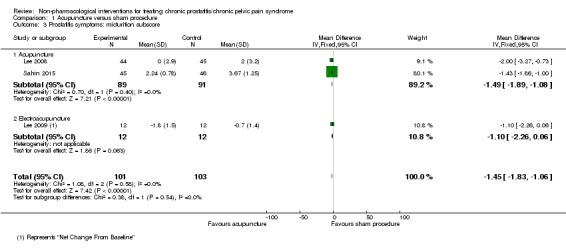
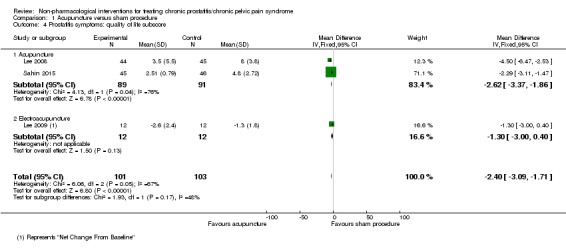
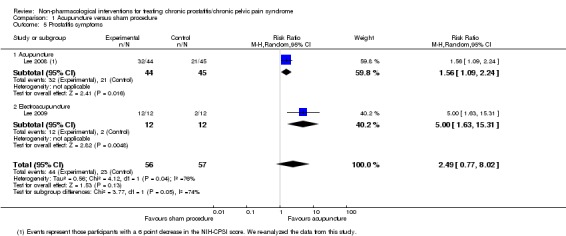
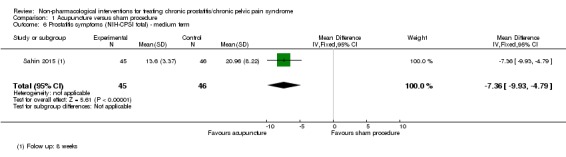
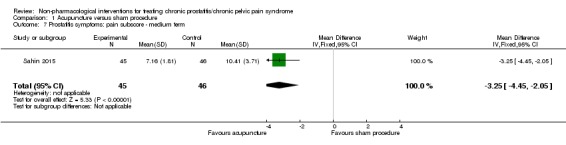
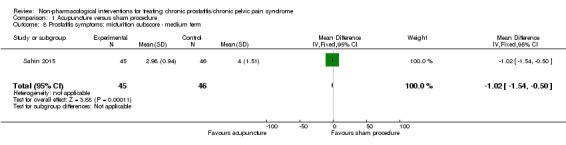
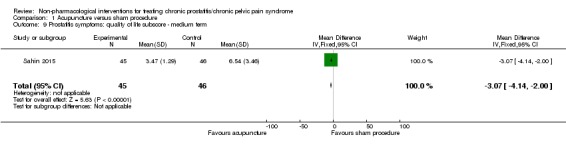
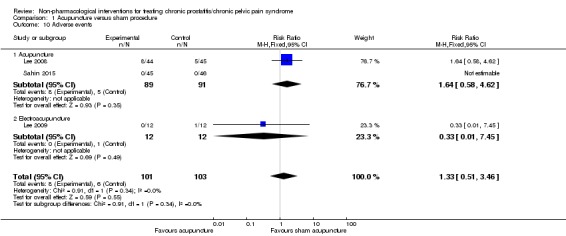
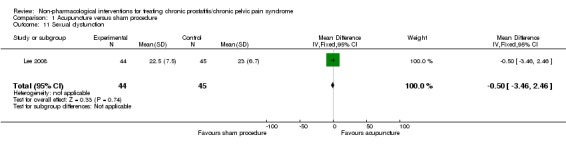
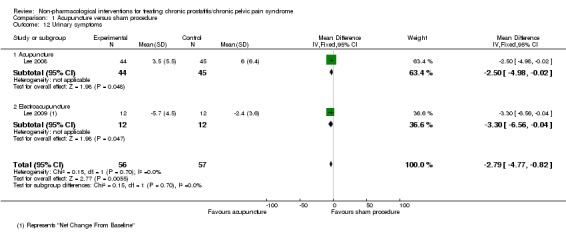
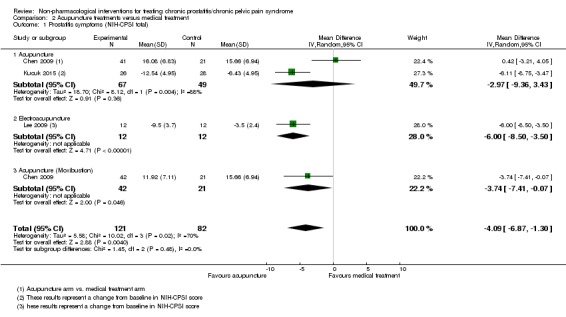
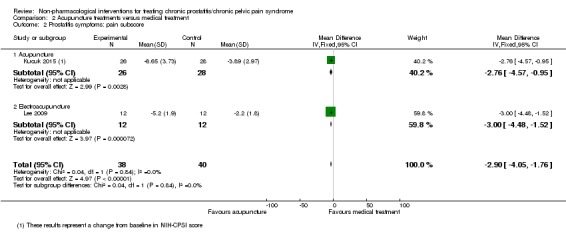
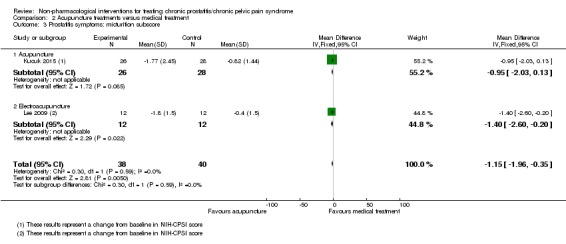
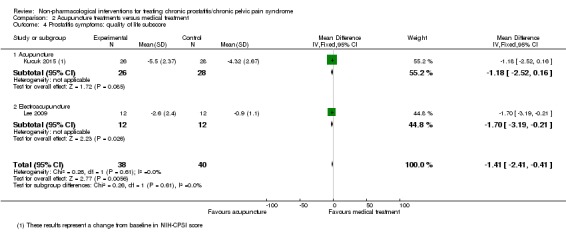
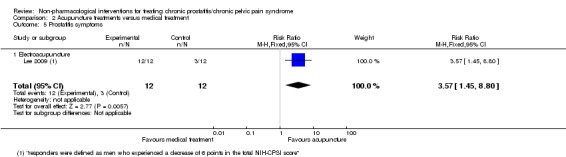
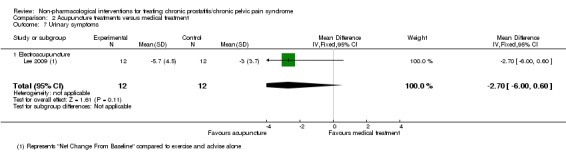
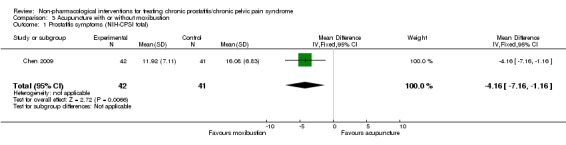
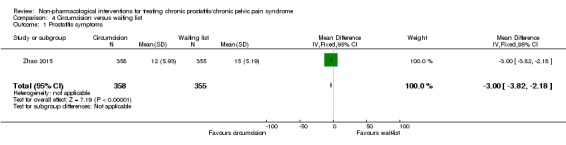
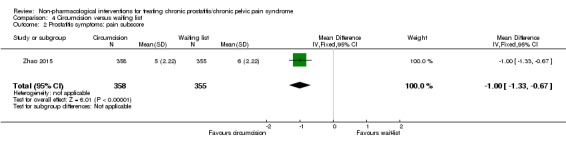
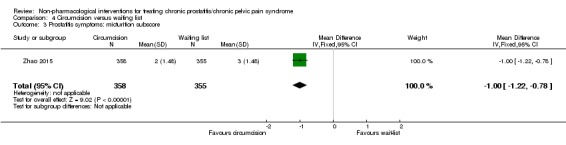
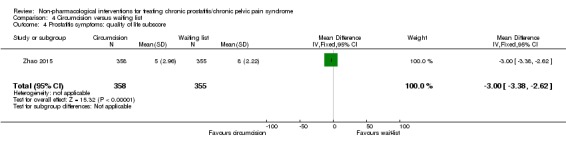
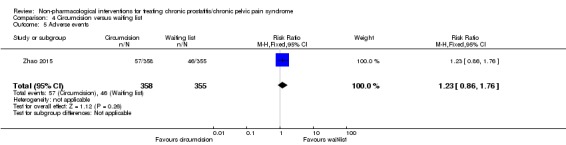
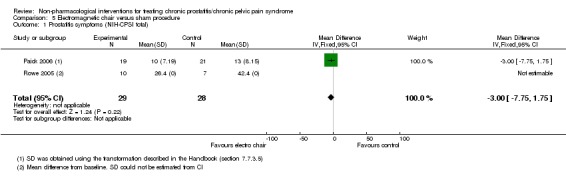
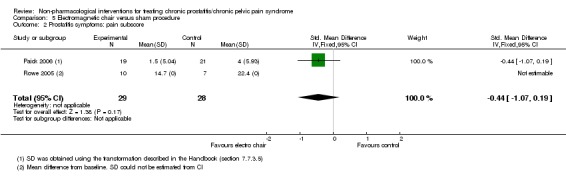
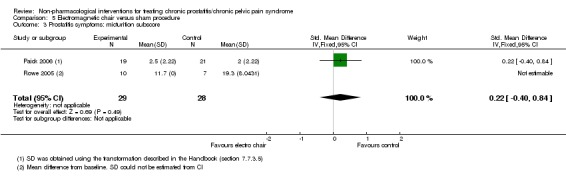
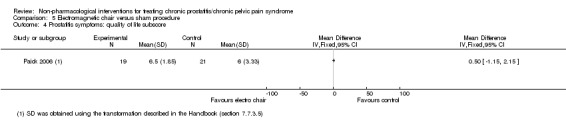
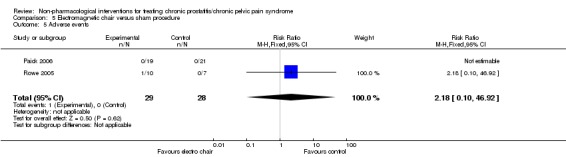
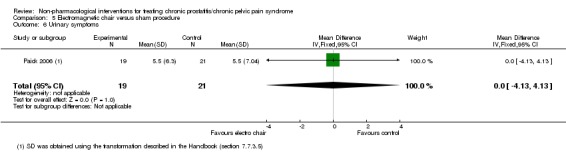
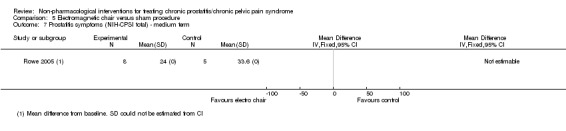
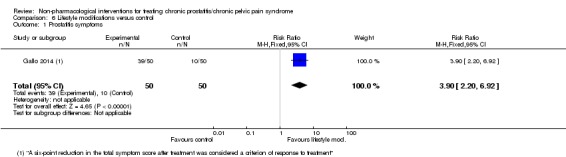
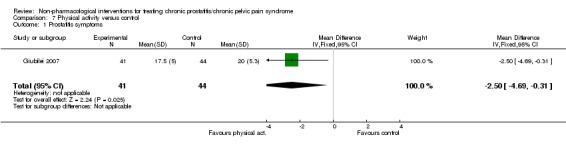
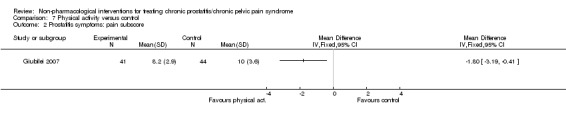
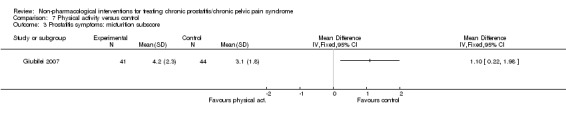
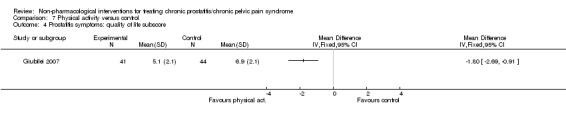
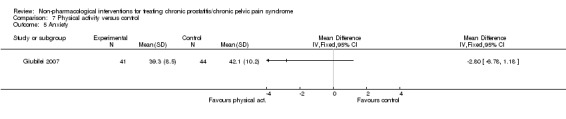
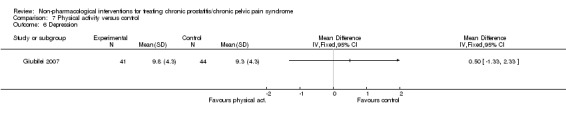
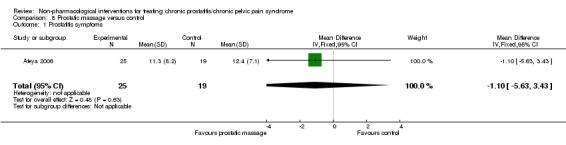
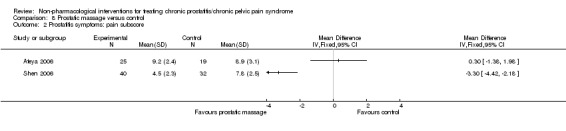
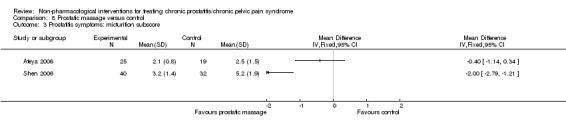
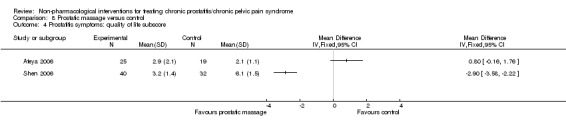
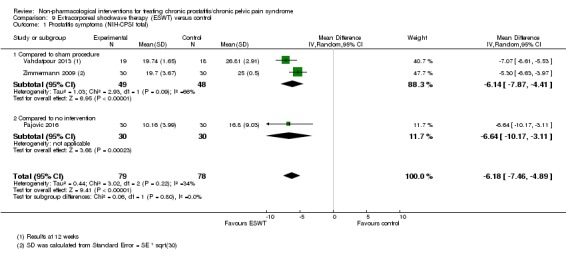
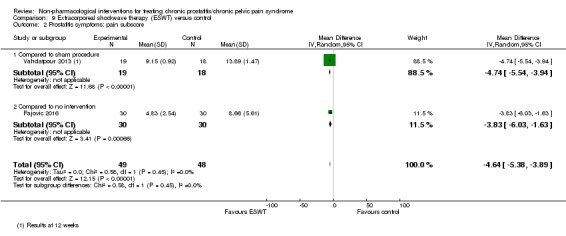
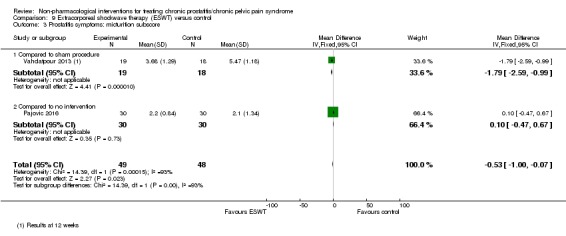
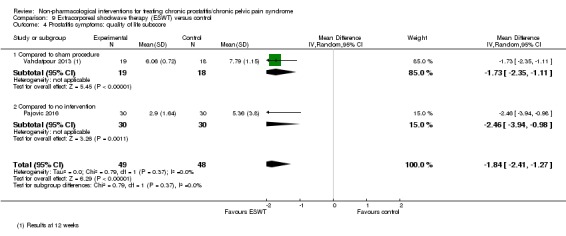
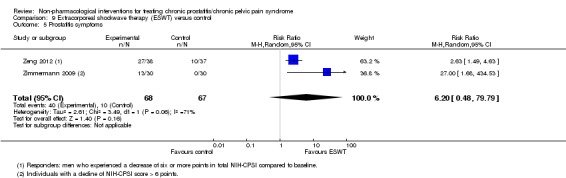
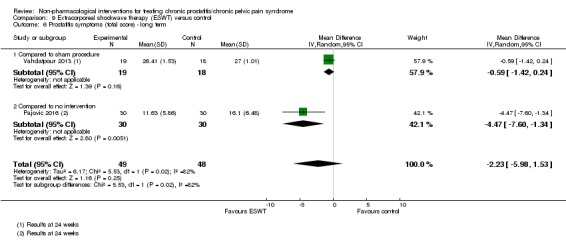
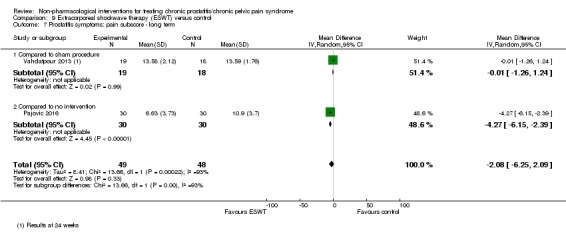
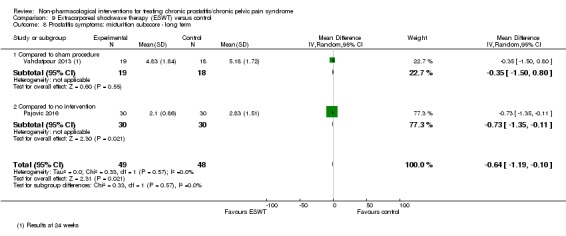
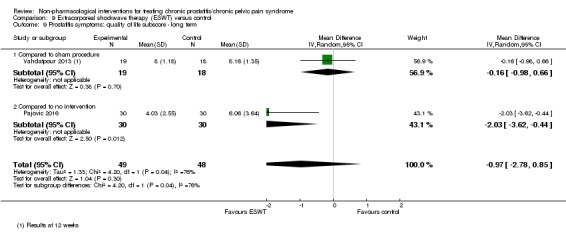
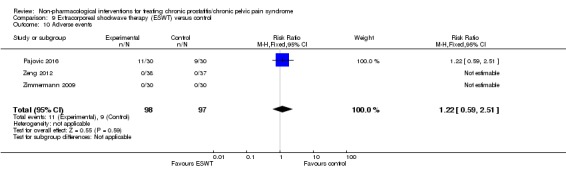
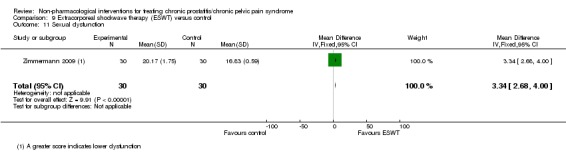
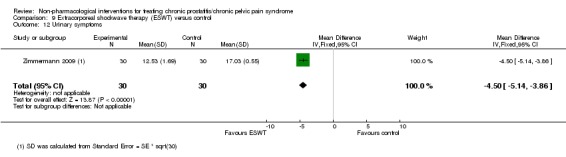
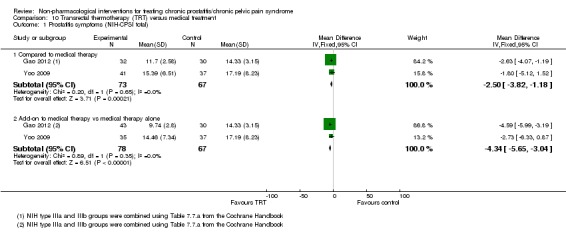
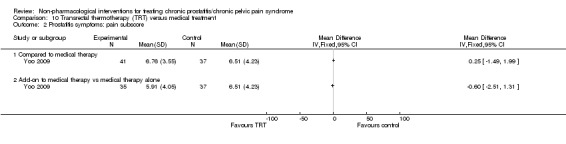
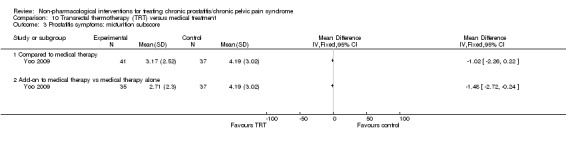
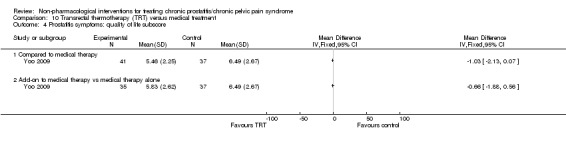
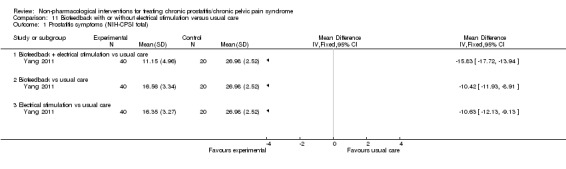
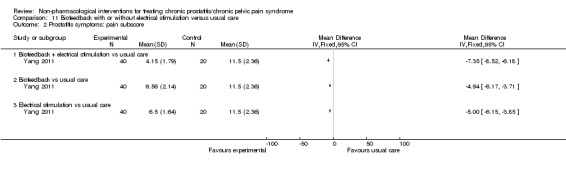
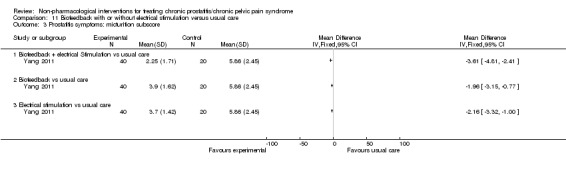
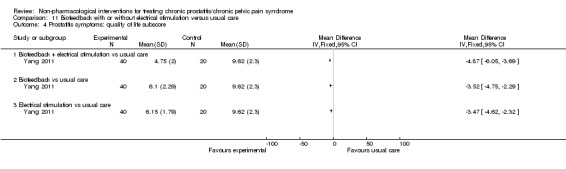
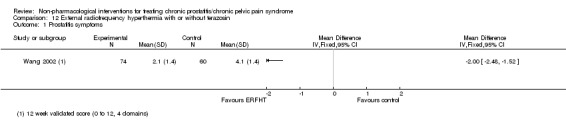
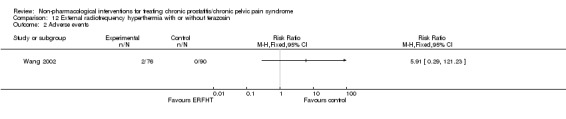
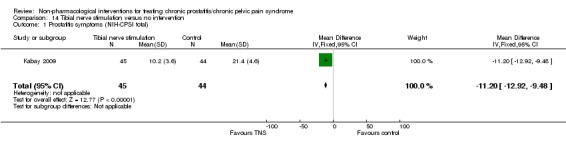
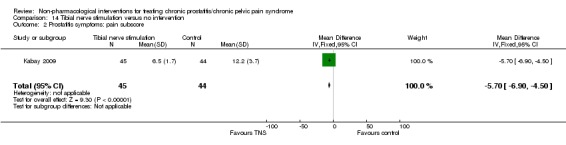
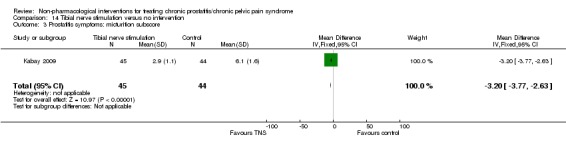
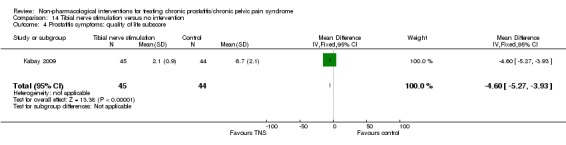
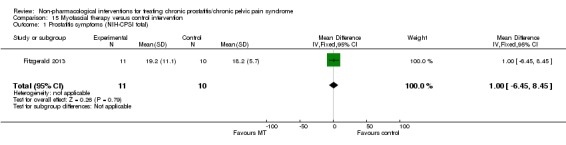
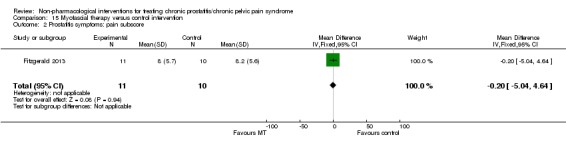
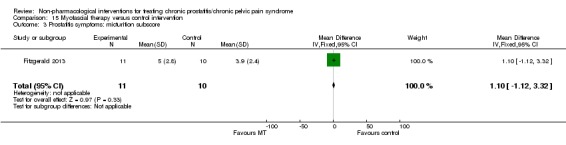
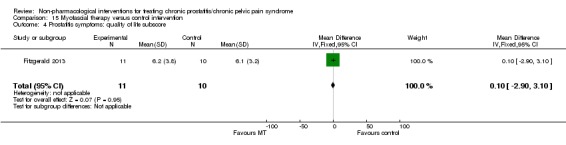
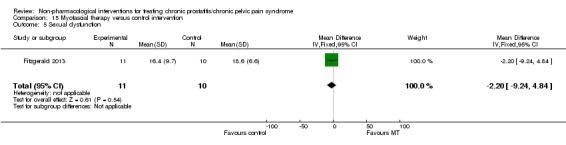
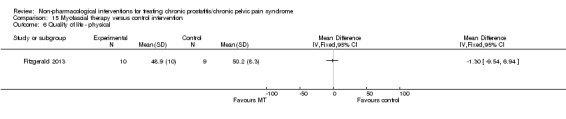
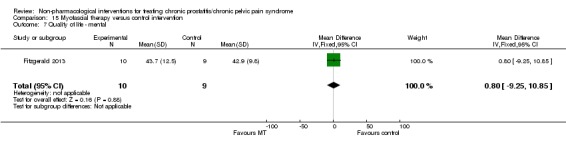
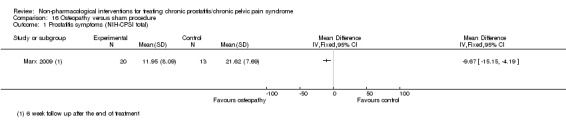
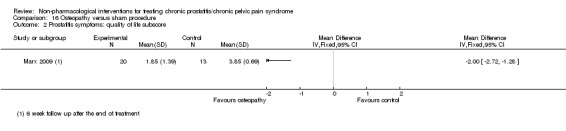
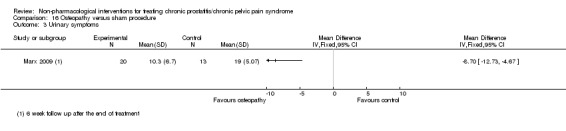
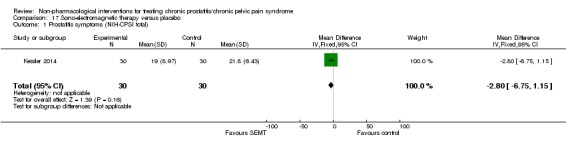
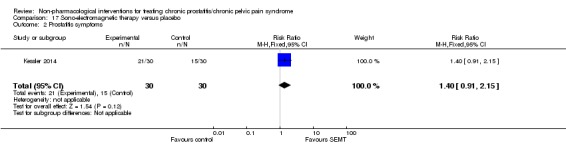
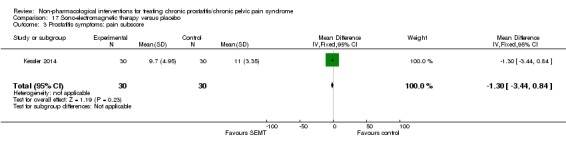
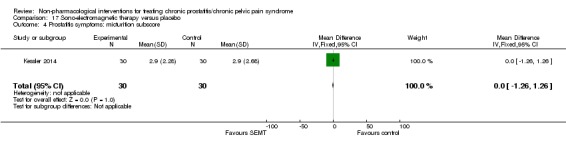
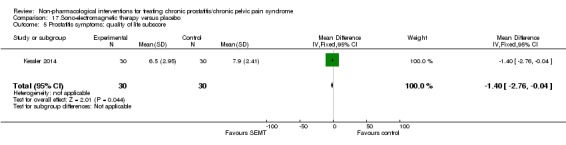
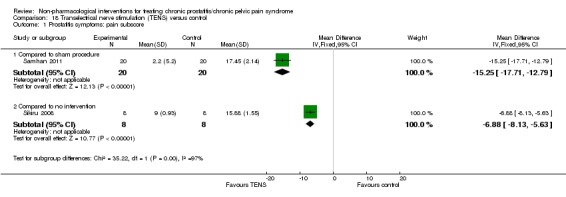
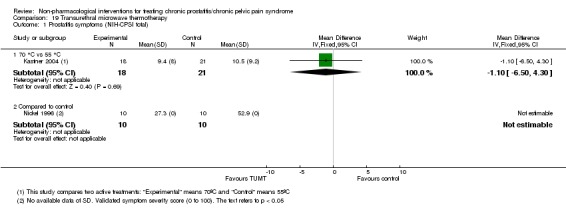
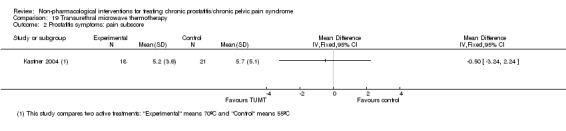
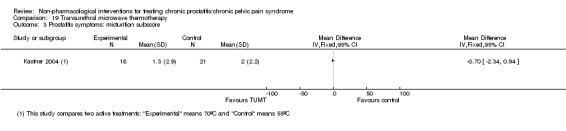
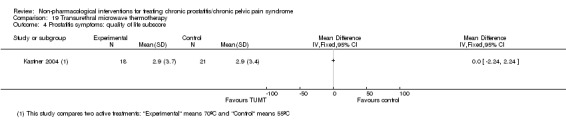
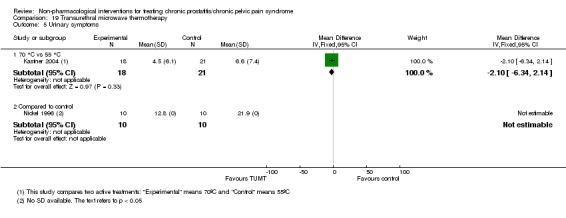
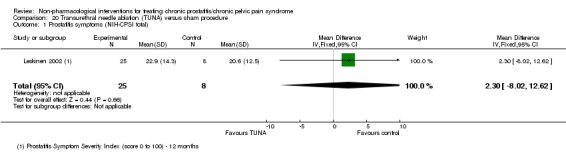
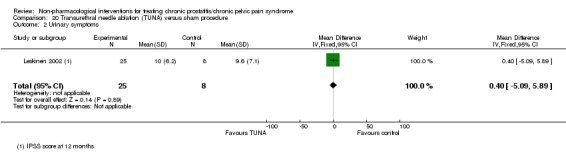
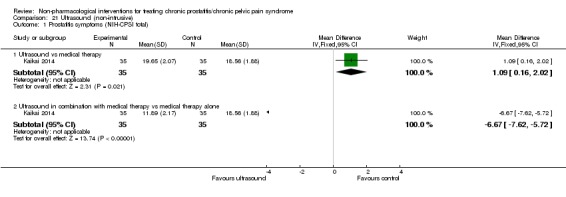
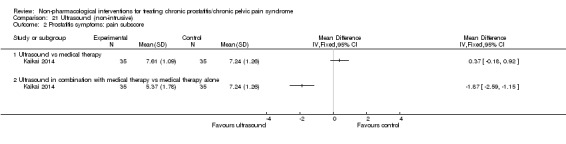
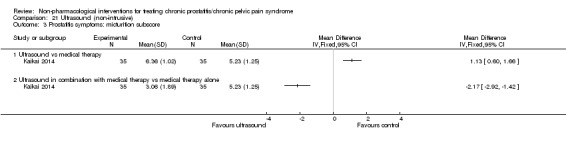
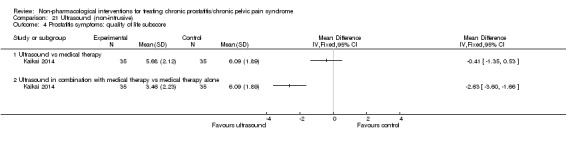
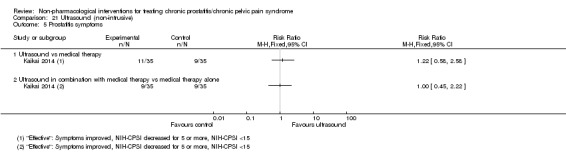
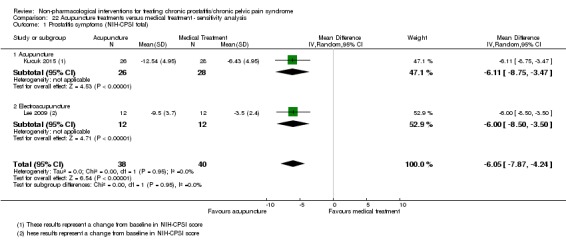
Main results: We included 38 unique studies with 3290 men with CP/CPPS across 23 comparisons.1. Acupuncture: (three studies, 204 participants) based on short-term follow-up, acupuncture reduces prostatitis symptoms in an appreciable number of participants compared with sham procedure (mean difference (MD) in total NIH-CPSI score -5.79, 95% confidence interval (CI) -7.32 to -4.26, high QoE). Acupuncture likely results in little to no difference in adverse events (moderate QoE). It probably also decreases prostatitis symptoms compared with standard medical therapy in an appreciable number of participants (MD -6.05, 95% CI -7.87 to -4.24, two studies, 78 participants, moderate QoE).2. Circumcision: (one study, 713 participants) based on short-term follow-up, early circumcision probably decreases prostatitis symptoms slightly (NIH-CPSI score MD -3.00, 95% CI -3.82 to -2.18, moderate QoE) and may not be associated with a greater incidence of adverse events compared with control (a waiting list to be circumcised, low QoE).3. Electromagnetic chair: (two studies, 57 participants) based on short-term follow-up, we are uncertain of the effects of the use of an electromagnetic chair on prostatitis symptoms. It may be associated with a greater incidence of adverse events compared with sham procedure (low to very low QoE).4. Lifestyle modifications: (one study, 100 participants) based on short-term follow-up, lifestyle modifications may be associated with a greater improvement in prostatitis symptoms in an appreciable number of participants compared with control (risk ratio (RR) for improvement in NIH-CPSI scores 3.90, 95% CI 2.20 to 6.92, very low QoE). We found no information regarding adverse events.5. Physical activity: (one study, 85 participants) based on short-term follow-up, a physical activity programme may cause a small reduction in prostatitis symptoms compared with control (NIH-CPSI score MD -2.50, 95% CI -4.69 to -0.31, low QoE). We found no information regarding adverse events.6. Prostatic massage: (two studies, 115 participants) based on short-term follow-up, we are uncertain whether the prostatic massage reduces or increases prostatitis symptoms compared with control (very low QoE). We found no information regarding adverse events.7. Extracorporeal shockwave therapy: (three studies, 157 participants) based on short-term follow-up, extracorporeal shockwave therapy reduces prostatitis symptoms compared with control (NIH-CPSI score MD -6.18, 95% CI -7.46 to -4.89, high QoE). These results may not be sustained at medium-term follow-up (low QoE). This treatment may not be associated with a greater incidence of adverse events (low QoE).8. Transrectal thermotherapy compared to medical therapy: (two studies, 237 participants) based on short-term follow-up, transrectal thermotherapy alone or in combination with medical therapy may decrease prostatitis symptoms slightly when compared with medical therapy alone (NIH-CPSI score MD -2.50, 95% CI -3.82 to -1.18, low QoE). One included study reported that participants may experience transient adverse events.9. Other interventions: there is uncertainty about the effects of other interventions included in this review. We found no information regarding psychological support or prostatic surgery.
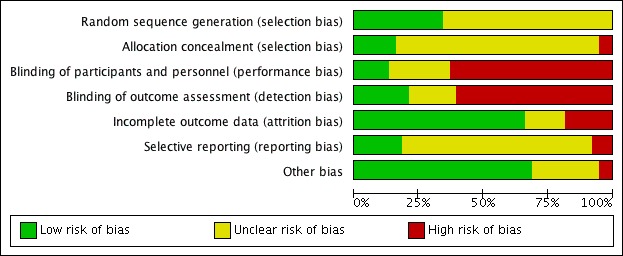
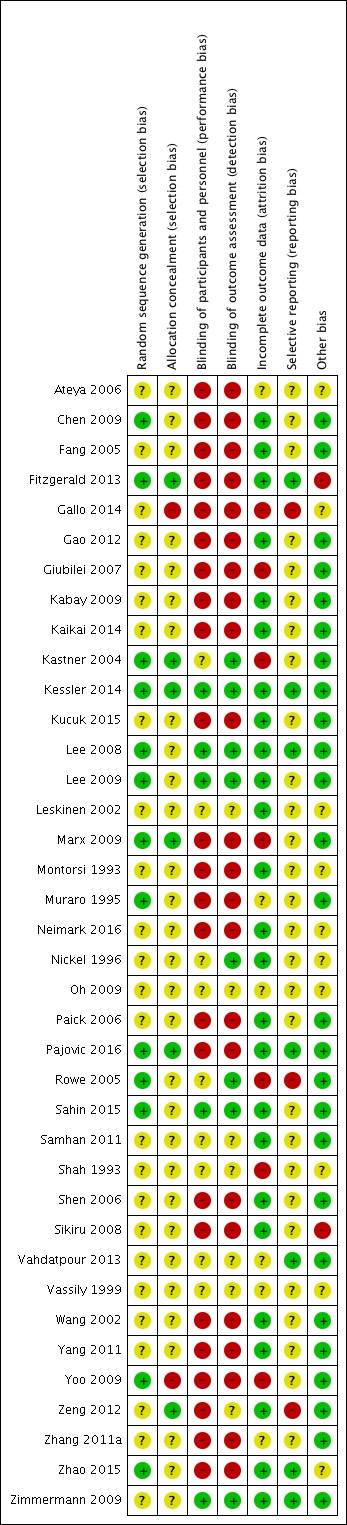
Authors' conclusions: Some of the interventions can decrease prostatitis symptoms in an appreciable number without a greater incidence of adverse events. The QoE was mostly low. Future clinical trials should include a full report of their methods including adequate masking, consistent assessment of all patient-important outcomes including potential treatment-related adverse events and appropriate sample sizes.
Conflict of interest statement
JVAF: none known.
TT: none known.
JHJ: none known.
YX: none known.
SI: none known.
VG: none known.
VV: none known.
Figures
References
References to studies included in this review
-
- Ateya A, Fayez A, Hani R, Zohdy W, Gabbar MA, Shamloul R. Evaluation of prostatic massage in treatment of chronic prostatitis. Urology 2006;67(4):674‐8. - PubMed
-
- Chen ZX. Observation on therapeutic effect of warm needle moxibustion on chronic non‐bacterial prostatitis. Zhongguo Zhen Jiu [Chinese Acupuncture & Moxibustion] 2009;29(4):275‐8. - PubMed
-
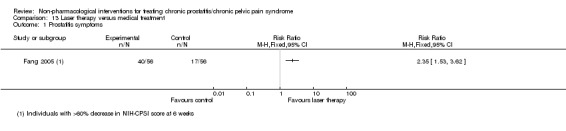
- Fang J, Xu G, Ding Q, Zhang Y‐F. Observation on the safety and efficacy of He‐Ne laser equipment on chronic abacteria prostatitis. Fudan University Journal of Medical Sciences 2005;32(2):234‐5, 252.
-
- Badillo SA, Neville CE, Kotarinos R, Fortman C, Fraser L, Cosby A, et al. Randomized multicenter pilot trial shows benefit of manual physical therapies in treatment of urologic chronic pelvic pain. Journal of Women's Health Physical Therapy 2009;33(1):23.
- FitzGerald MP, Anderson RU, Potts J, Payne CK, Peters KM, Clemens JQ, et al. Randomized multicenter feasibility trial of myofascial physical therapy for the treatment of urological chronic pelvic pain syndromes. Journal of Urology 2009;182(2):570‐80. - PMC - PubMed
- Fitzgerald MP, Anderson RU, Potts J, Payne CK, Peters KM, Clemens JQ, et al. Randomized multicenter feasibility trial of myofascial physical therapy for the treatment of urological chronic pelvic pain syndromes. Journal of Urology 2013;189(1 Suppl):S75‐85. - PMC - PubMed
-
- Gallo L. Effectiveness of diet, sexual habits and lifestyle modifications on treatment of chronic pelvic pain syndrome. Prostate Cancer and Prostatic Diseases 2014;17(3):238‐45. - PubMed
References to studies excluded from this review
-
- Aliaev IuG, Vinarov AZ, Lokshin KL, Spivak LG. Efficiency and safety of prostamol‐Uno in patients with chronic abacterial prostatitis. Urologiia 2006;1(1):47‐50. - PubMed
-
- Allen S, Aghajanyan IG. Effect of thermobalancing therapy on chronic prostatitis and chronic pelvic pain syndrome. Journal of Clinical Urology 2017;10(4):347‐54.
- Allen S, Aghajanyan IG. New independent thermobalancing treatment with therapeutic device for chronic prostatitis/chronic pelvic pain syndrome. Nephro‐Urology Monthly 2017;9(2):1‐6.
-
- Anothaisintawee T, Attia J, Nickel JC, Thammakraisorn S, Numthavaj P, McEvoy M, et al. Management of chronic prostatitis/chronic pelvic pain syndrome: a systematic review and network meta‐analysis. JAMA 2011;305(1):78‐86. - PubMed
-
- Barbalias GA, Nikiforidis G, Liatsikos EN. Alpha‐blockers for the treatment of chronic prostatitis in combination with antibiotics. Urologia Internationalis 1998;159(3):883‐7. - PubMed
References to studies awaiting assessment
References to ongoing studies
-
- ChiCTR‐IPR‐16009262. A randomized controlled trial of psychological intervention therapy in patients with category III chronic prostatitis/chronic pelvic pain syndrome. http://www.chictr.org.cn/showprojen.aspx?proj=15638 (accessed 22 January....
-
- Shocking Therapy for Chronic Pelvic Pain Syndrome (CPPS).. Ongoing studyFebruary 2013..
-
- NCT03213938. Acupuncture for chronic prostatitis/chronic pelvic pain syndrome: a multicenter randomized controlled trial. clinicaltrials.gov/ct2/show/NCT03213938 Date first registered: 11 July 2017.
Additional references
-
- Alonso‐Coello P, Schünemann HJ, Moberg J, Brignardello‐Petersen R, Akl EA, Davoli M, et al. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ (Clinical Research Ed.) 2016;353:i2016. [PUBMED: 27353417] - PubMed
-
- Antolak SJ Jr, Hough DM, Pawlina W, Spinner RJ. Anatomical basis of chronic pelvic pain syndrome: the ischial spine and pudendal nerve entrapment. Medical Hypotheses 2002;59(3):349‐53. [PUBMED: 12208168] - PubMed
-
- Arisan ED, Arisan S, Kiremit MC, Tigli H, Caskurlu T, Palavan‐Unsal N, et al. Manganese superoxide dismutase polymorphism in chronic pelvic pain syndrome patients. Prostate Cancer and Prostatic Diseases 2006;9(4):426‐31. [PUBMED: 16847469] - PubMed
-
- Bajpayee P, Kumar K, Sharma S, Maurya N, Kumar P, Singh R, et al. Prostatitis: prevalence, health impact and quality improvement strategies. Acta Poloniae Pharmaceutica 2012;69(4):571‐9. [PUBMED: 22876597] - PubMed
References to other published versions of this review
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous