

Comparison of Compressive Myofascial Release and the Graston Technique for Improving Ankle-Dorsiflexion Range of Motion
- PMID: 29373060
- PMCID: PMC5842906
- DOI: 10.4085/1062-6050-386-16
Comparison of Compressive Myofascial Release and the Graston Technique for Improving Ankle-Dorsiflexion Range of Motion
Abstract
Context: Restricted dorsiflexion (DF) at the ankle joint can cause acute and chronic injuries at the ankle and knee. Myofascial release and instrument-assisted soft tissue mobilization (IASTM) techniques have been used to increase range of motion (ROM); however, evidence directly comparing their effectiveness is limited.
Objective: To compare the effects of a single session of compressive myofascial release (CMR) or IASTM using the Graston Technique (GT) on closed chain ankle-DF ROM.
Design: Randomized controlled trial.
Setting: Laboratory.
Patients or other participants: Participants were 44 physically active people (53 limbs) with less than 30° of DF.
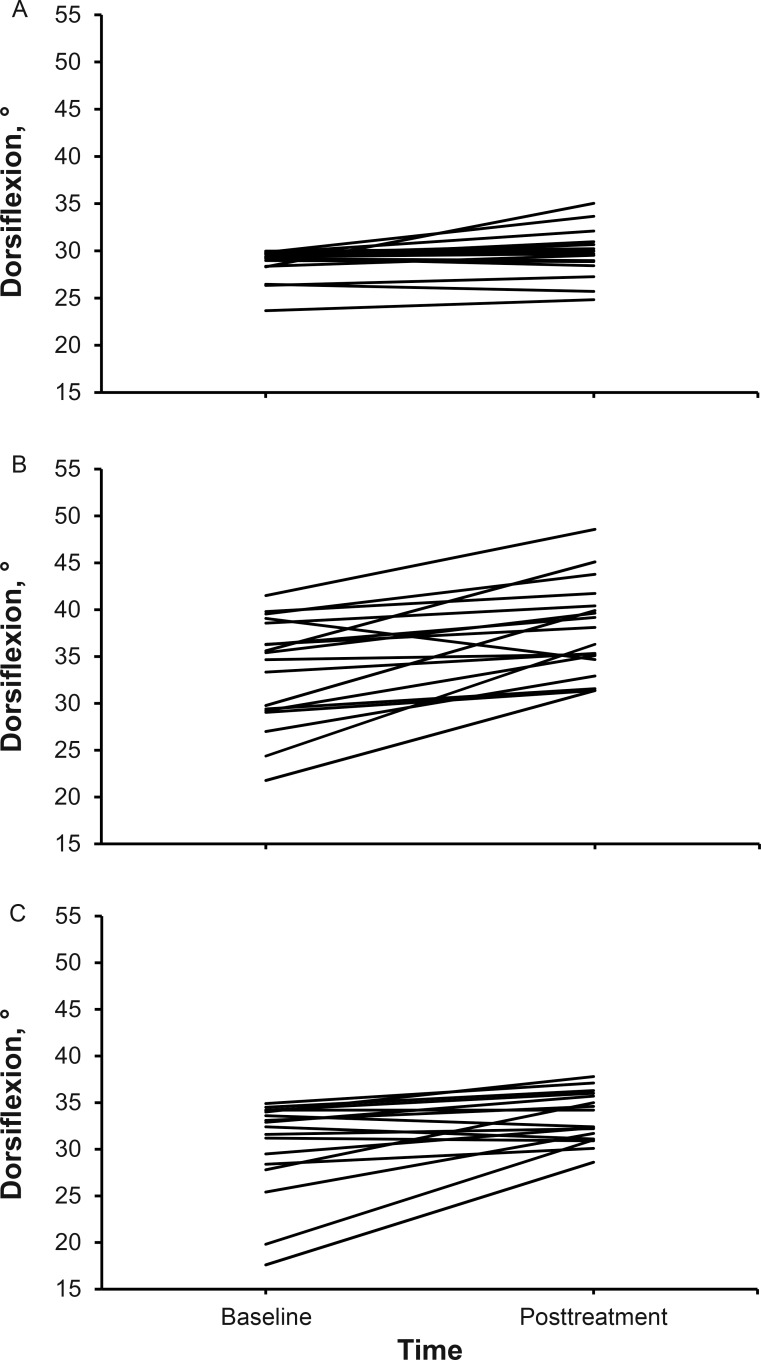
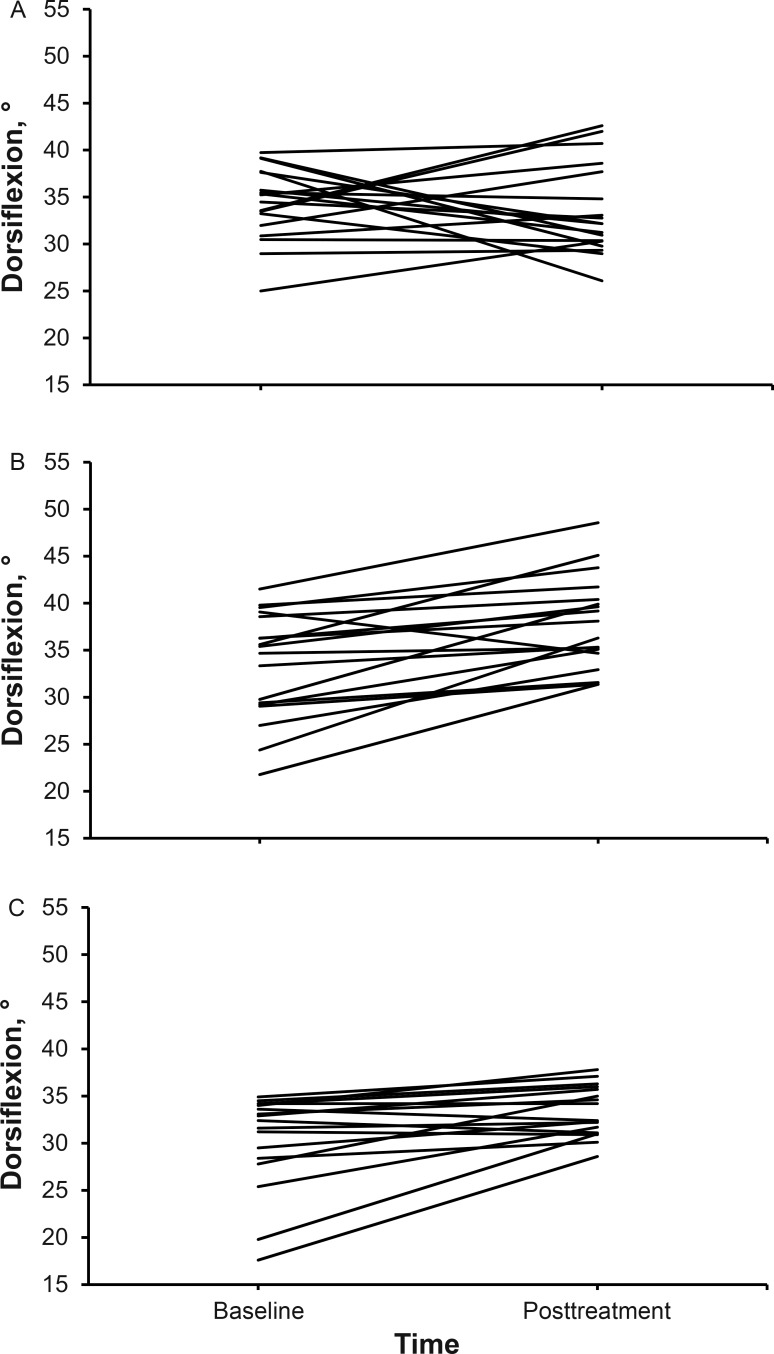
Intervention(s): Limbs were randomly assigned to 1 of 3 groups: control, CMR, or GT. Both treatment groups received one 5-minute treatment that included scanning the area and treating specific restrictions. The control group sat for 5 minutes before measurements were retaken.
Main outcome measure(s): Standing and kneeling ankle DF were measured before and immediately after treatment. Change scores were calculated for both positions, and two 1-way analyses of variance were conducted.
Results: A difference between groups was found in the standing ( F2,52 = 13.78, P = .001) and kneeling ( F2,52 = 5.85, P = .01) positions. Post hoc testing showed DF improvements in the standing position after CMR compared with the GT and control groups (both P = .001). In the kneeling position, DF improved after CMR compared with the control group ( P = .005).
Conclusions: Compressive myofascial release increased ankle DF after a single treatment in participants with DF ROM deficits. Clinicians should consider adding CMR as a treatment intervention for patients with DF deficits.
Keywords: manual therapy; muscle tightness; soft tissue mobilization.
Figures




Comment in
-
Letter to the Editor.J Athl Train. 2018 Jul;53(7):633-634. doi: 10.4085/1062-6050-53-01. J Athl Train. 2018. PMID: 30192677 Free PMC article. No abstract available.
References
-
- You JY, Lee HM, Luo HJ, Lee CC, Cheng PG, Wu SK. . Gastrocnemius tightness on joint angle and work of lower extremity during gait. Clin Biomech (Bristol, Avon). 2009; 24 9: 744– 750. - PubMed
-
- Willems TM, Witvrouw E, Delbaere K, De Bourdeaudhuij I, De Clercq D. . Intrinsic risk factors for inversion ankle sprains in male subjects: a prospective study. Am J Sports Med. 2005; 33 3: 415– 423. - PubMed
-
- Reid A, Birmingham T, Alcock G. . Efficacy of mobilization with movement for patients with limited dorsiflexion after ankle sprain: a crossover trial. Physiother Can. 2007; 59 3: 166– 172.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
