

Acute Kidney Injury and Subsequent Frailty Status in Survivors of Critical Illness: A Secondary Analysis
- PMID: 29373362
- PMCID: PMC5899022
- DOI: 10.1097/CCM.0000000000003003
Acute Kidney Injury and Subsequent Frailty Status in Survivors of Critical Illness: A Secondary Analysis
Abstract
Objectives: Acute kidney injury frequently complicates critical illness and is associated with high morbidity and mortality. Frailty is common in critical illness survivors, but little is known about the impact of acute kidney injury. We examined the association of acute kidney injury and frailty within a year of hospital discharge in survivors of critical illness.
Design: Secondary analysis of a prospective cohort study.
Setting: Medical/surgical ICU of a U.S. tertiary care medical center.
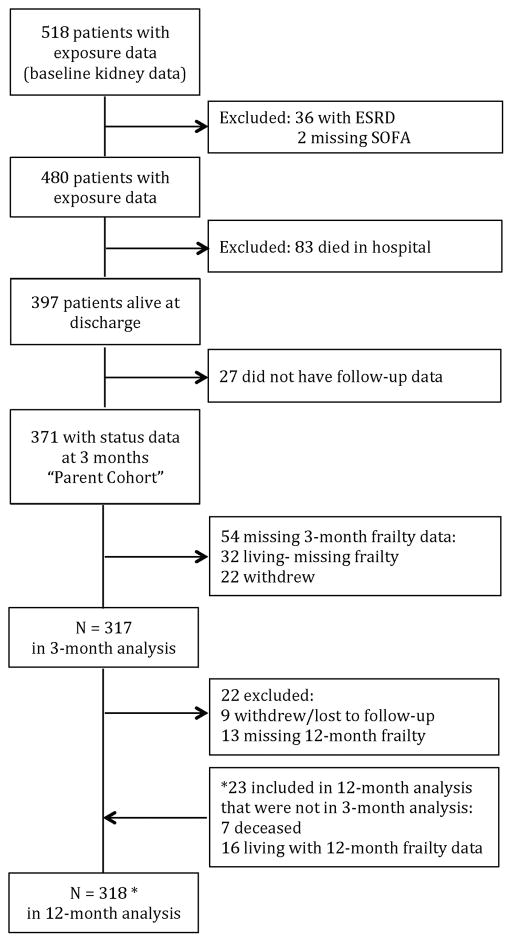
Patients: Three hundred seventeen participants with respiratory failure and/or shock.
Interventions: None.
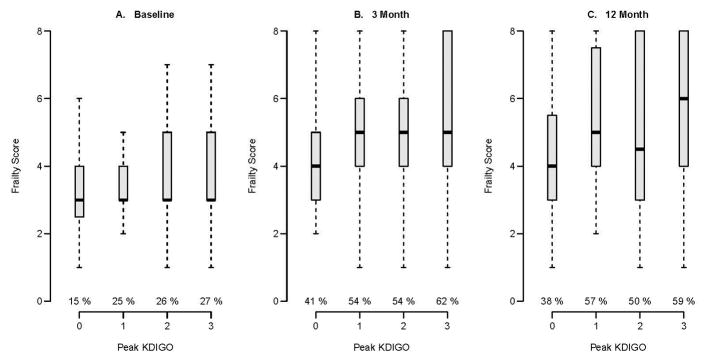
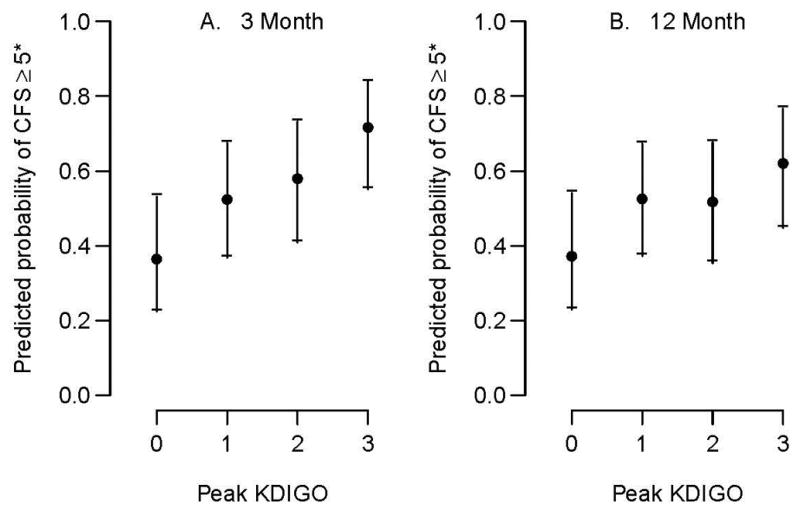
Measurements and main results: Acute kidney injury was determined using Kidney Disease Improving Global Outcomes stages. Clinical frailty status was determined using the Clinical Frailty Scale at 3 and 12 months following discharge. Covariates included mean ICU Sequential Organ Failure Assessment score and Acute Physiology and Chronic Health Evaluation II score as well as baseline comorbidity (i.e., Charlson Comorbidity Index), kidney function, and Clinical Frailty Scale score. Of 317 patients, 243 (77%) had acute kidney injury and one in four patients with acute kidney injury was frail at baseline. In adjusted models, acute kidney injury stages 1, 2, and 3 were associated with higher frailty scores at 3 months (odds ratio, 1.92; 95% CI, 1.14-3.24; odds ratio, 2.40; 95% CI, 1.31-4.42; and odds ratio, 4.41; 95% CI, 2.20-8.82, respectively). At 12 months, a similar association of acute kidney injury stages 1, 2, and 3 and higher Clinical Frailty Scale score was noted (odds ratio, 1.87; 95% CI, 1.11-3.14; odds ratio, 1.81; 95% CI, 0.94-3.48; and odds ratio, 2.76; 95% CI, 1.34-5.66, respectively). In supplemental and sensitivity analyses, analogous patterns of association were observed.
Conclusions: Acute kidney injury in survivors of critical illness predicted worse frailty status 3 and 12 months postdischarge. These findings have important implications on clinical decision making among acute kidney injury survivors and underscore the need to understand the drivers of frailty to improve patient-centered outcomes.
Conflict of interest statement
The authors have no conflicts to declare.
Figures
Comment in
-
The impact of acute kidney injury on frailty status in critical illness survivors-is there enough evidence?J Emerg Crit Care Med. 2018 Nov;2:93. doi: 10.21037/jeccm.2018.10.17. Epub 2018 Nov 7. J Emerg Crit Care Med. 2018. PMID: 30662978 Free PMC article. No abstract available.
References
-
- Cerda J, Lameire N, Eggers P, et al. Epidemiology of acute kidney injury. Clin J Am Soc Nephrol. 2008;3(3):881–886. - PubMed
-
- Pisoni R, Wille KM, Tolwani AJ. The epidemiology of severe acute kidney injury: from BEST to PICARD, in acute kidney injury: new concepts. Nephron Clin Pract. 2008;109(4):c188–191. - PubMed
-
- Waikar SS, Liu KD, Chertow GM. Diagnosis, epidemiology and outcomes of acute kidney injury. Clin J Am Soc Nephrol. 2008;3(3):844–861. - PubMed
-
- Rewa O, Bagshaw SM. Acute kidney injury-epidemiology, outcomes and economics. Nature reviews Nephrology. 2014;10(4):193–207. - PubMed
-
- Villeneuve PM, Clark EG, Sikora L, et al. Health-related quality-of-life among survivors of acute kidney injury in the intensive care unit: a systematic review. Intensive care medicine. 2016;42(2):137–146. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
