

Early low-anticoagulant desulfated heparin after traumatic brain injury: Reduced brain edema and leukocyte mobilization is associated with improved watermaze learning ability weeks after injury
- PMID: 29373460
- PMCID: PMC9380841
- DOI: 10.1097/TA.0000000000001819
Early low-anticoagulant desulfated heparin after traumatic brain injury: Reduced brain edema and leukocyte mobilization is associated with improved watermaze learning ability weeks after injury
Abstract
Background: Unfractionated heparin administered immediately after traumatic brain injury (TBI) reduces brain leukocyte (LEU) accumulation, and enhances early cognitive recovery, but may increase bleeding after injury. It is unknown how non-anticoagulant heparins, such as 2,3-O desulfated heparin (ODSH), impact post-TBI cerebral inflammation and long-term recovery. We hypothesized that ODSH after TBI reduces LEU-mediated brain inflammation and improves long-term neurologic recovery.
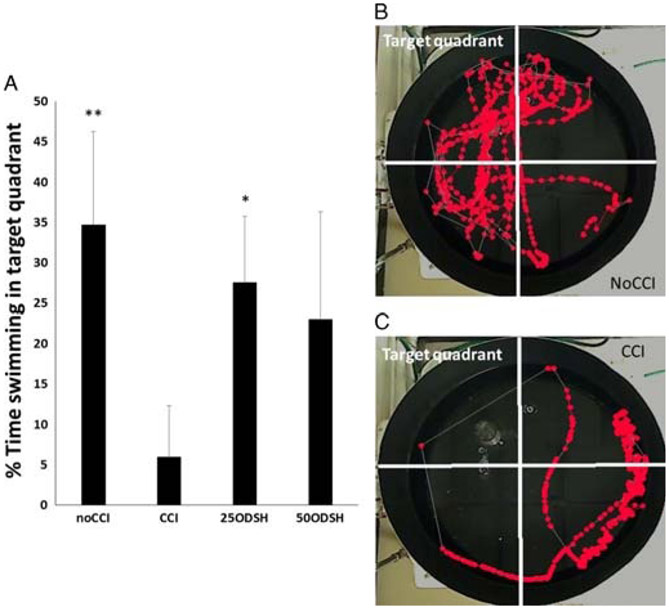
Methods: CD1 male mice (n = 66) underwent either TBI (controlled cortical impact [CCI]) or sham craniotomy. 2,3-O desulfated heparin (25 mg/kg [25ODSH] or 50 mg/kg [50ODSH]) or saline was administered for 48 hours after TBI in 46 animals. At 48 hours, intravital microscopy visualized rolling LEUs and fluorescent albumin leakage in the pial circulation, and the Garcia Neurologic Test assessed neurologic function. Brain edema (wet/dry ratio) was evaluated post mortem. In a separate group of animals (n = 20), learning/memory ability (% time swimming in the Probe platform quadrant) was assessed by the Morris Water Maze 17 days after TBI. Analysis of variance with Bonferroni correction determined significance (p < 0.05).
Results: Compared with CCI (LEU rolling: 32.3 ± 13.7 LEUs/100 μm per minute, cerebrovascular albumin leakage: 57.4 ± 5.6%), both ODSH doses reduced post-TBI pial LEU rolling (25ODSH: 18.5 ± 9.2 LEUs/100 μm per minute, p = 0.036; 50ODSH: 7.8 ± 3.9 LEUs/100 μm per minute, p < 0.001) and cerebrovascular albumin leakage (25ODSH: 37.9 ± 11.7%, p = 0.001, 50ODSH: 32.3 ± 8.7%, p < 0.001). 50ODSH also reduced injured cerebral hemisphere edema (77.7 ± 0.4%) vs. CCI (78.7 ± 0.4 %, p = 0.003). Compared with CCI, both ODSH doses improved Garcia Neurologic Test at 48 hours. Learning/memory ability (% time swimming in target quadrant) was lowest in CCI (5.9 ± 6.4%) and significantly improved in the 25ODSH group (27.5 ± 8.2%, p = 0.025).
Conclusion: 2,3-O desulfated heparin after TBI reduces cerebral LEU recruitment, microvascular permeability and edema. 2,3-O desulfated heparin may also improve acute neurologic recovery leading to improved learning/memory ability weeks after injury.
Conflict of interest statement
DISCLOSURE
The authors declare no conflicts of interest.
Figures





Similar articles
-
Unfractionated heparin after TBI reduces in vivo cerebrovascular inflammation, brain edema and accelerates cognitive recovery.J Trauma Acute Care Surg. 2016 Dec;81(6):1088-1094. doi: 10.1097/TA.0000000000001215. J Trauma Acute Care Surg. 2016. PMID: 27533909 Free PMC article.
-
Early heparin administration after traumatic brain injury: Prolonged cognitive recovery associated with reduced cerebral edema and neutrophil sequestration.J Trauma Acute Care Surg. 2017 Sep;83(3):406-412. doi: 10.1097/TA.0000000000001590. J Trauma Acute Care Surg. 2017. PMID: 28538627 Free PMC article.
-
Enoxaparin ameliorates post-traumatic brain injury edema and neurologic recovery, reducing cerebral leukocyte endothelial interactions and vessel permeability in vivo.J Trauma Acute Care Surg. 2015 Jul;79(1):78-84. doi: 10.1097/TA.0000000000000697. J Trauma Acute Care Surg. 2015. PMID: 26091318 Free PMC article.
-
Neuroprotective profile of enoxaparin, a low molecular weight heparin, in in vivo models of cerebral ischemia or traumatic brain injury in rats: a review.CNS Drug Rev. 2002 Spring;8(1):1-30. doi: 10.1111/j.1527-3458.2002.tb00213.x. CNS Drug Rev. 2002. PMID: 12070524 Free PMC article. Review.
-
Elucidating opportunities and pitfalls in the treatment of experimental traumatic brain injury to optimize and facilitate clinical translation.Neurosci Biobehav Rev. 2018 Feb;85:160-175. doi: 10.1016/j.neubiorev.2017.05.022. Epub 2017 May 30. Neurosci Biobehav Rev. 2018. PMID: 28576511 Free PMC article. Review.
Cited by
-
Multi-target approaches to CNS repair: olfactory mucosa-derived cells and heparan sulfates.Nat Rev Neurol. 2020 Apr;16(4):229-240. doi: 10.1038/s41582-020-0311-0. Epub 2020 Feb 25. Nat Rev Neurol. 2020. PMID: 32099190 Review.
-
Leukocyte Heparanase: A Double-Edged Sword in Tumor Progression.Front Oncol. 2019 Apr 29;9:331. doi: 10.3389/fonc.2019.00331. eCollection 2019. Front Oncol. 2019. PMID: 31110966 Free PMC article. Review.
-
HMGB1 Inhibition to Ameliorate Organ Failure and Increase Survival in Trauma.Biomolecules. 2022 Jan 8;12(1):101. doi: 10.3390/biom12010101. Biomolecules. 2022. PMID: 35053249 Free PMC article.
-
The role of autoimmunity in pituitary dysfunction due to traumatic brain injury.Pituitary. 2019 Jun;22(3):236-248. doi: 10.1007/s11102-019-00953-z. Pituitary. 2019. PMID: 30847776 Review.
-
The Use of Myelinating Cultures as a Screen of Glycomolecules for CNS Repair.Biology (Basel). 2019 Jun 28;8(3):52. doi: 10.3390/biology8030052. Biology (Basel). 2019. PMID: 31261710 Free PMC article.
References
-
- Kerr ZY, Harmon KJ, Marshall SW, Proescholdbell SK, Waller AE. The epidemiology of traumatic brain injuries treated in emergency departments in North Carolina, 2010-2011. N C Med J. 2014;75(1):8–14. - PubMed
-
- Scholz M, Cinatl J, Schadel-Hopfner M, Windolf J. Neutrophils and the blood-brain barrier dysfunction after trauma. Med Res Rev. 2007;27(3):401–416. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
