

Does Extracorporeal Membrane Oxygenation Improve Survival in Pediatric Acute Respiratory Failure?
- PMID: 29373797
- PMCID: PMC6019927
- DOI: 10.1164/rccm.201709-1893OC
Does Extracorporeal Membrane Oxygenation Improve Survival in Pediatric Acute Respiratory Failure?
Abstract
Rationale: Extracorporeal membrane oxygenation (ECMO) has supported gas exchange in children with severe respiratory failure for more than 40 years, without ECMO efficacy studies.
Objectives: To compare the mortality and functional status of children with severe acute respiratory failure supported with and without ECMO.
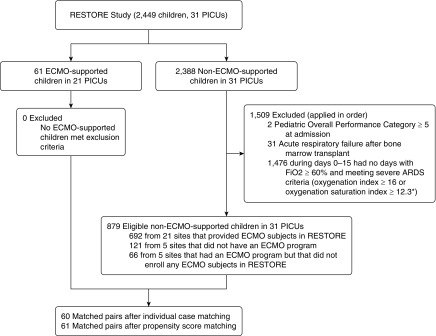
Methods: This cohort study compared ECMO-supported children to pair-matched non-ECMO-supported control subjects with severe acute respiratory distress syndrome (ARDS). Both individual case matching and propensity score matching were used. The study sample was selected from children enrolled in the cluster-randomized RESTORE (Randomized Evaluation of Sedation Titration for Respiratory Failure) clinical trial. Detailed demographic and daily physiologic data were used to match patients. The primary endpoint was in-hospital mortality. Secondary outcomes included hospital-free days, ventilator-free days, and change in functional status at hospital discharge.
Measurements and main results: Of 2,449 children in the RESTORE trial, 879 (35.9%) non-ECMO-supported patients with severe ARDS were eligible to match to 61 (2.5%) ECMO-supported children. When individual case matching was used (60 matched pairs), the in-hospital mortality rate at 90 days was 25% (15 of 60) for both the ECMO-supported and non-ECMO-supported children (P > 0.99). With propensity score matching (61 matched pairs), the ECMO-supported in-hospital mortality rate was 15 of 61 (25%), and the non-ECMO-supported hospital mortality rate was 18 of 61 (30%) (P = 0.70). There was no difference between ECMO-supported and non-ECMO-supported patients in any secondary outcomes.
Conclusions: In children with severe ARDS, our results do not demonstrate that ECMO-supported children have superior outcomes compared with non-ECMO-supported children. Definitive answers will require a rigorous multisite randomized controlled trial.
Keywords: acute respiratory distress syndrome; extracorporeal life support; extracorporeal membrane oxygenation; pediatric acute respiratory distress syndrome; propensity score analysis.
Figures
Comment in
-
Waiting for Godot: Clinical Trials of Extracorporeal Membrane Oxygenation for Pediatric Respiratory Failure.Am J Respir Crit Care Med. 2018 May 1;197(9):1103-1104. doi: 10.1164/rccm.201802-0268ED. Am J Respir Crit Care Med. 2018. PMID: 29522693 No abstract available.
-
Reply to Rambaud et al.: Do We Really Doubt Extracorporeal Membrane Oxygenation Efficacy in Pediatric Acute Respiratory Distress Syndrome?Am J Respir Crit Care Med. 2018 Aug 1;198(3):409-410. doi: 10.1164/rccm.201803-0459LE. Am J Respir Crit Care Med. 2018. PMID: 29617573 Free PMC article. No abstract available.
-
Do We Really Doubt Extracorporeal Membrane Oxygenation Efficacy in Pediatric Acute Respiratory Distress Syndrome?Am J Respir Crit Care Med. 2018 Aug 1;198(3):408-409. doi: 10.1164/rccm.201802-0221LE. Am J Respir Crit Care Med. 2018. PMID: 29617575 No abstract available.
References
-
- Bartlett RH, Gazzaniga AB, Jefferies MR, Huxtable RF, Haiduc NJ, Fong SW. Extracorporeal membrane oxygenation (ECMO) cardiopulmonary support in infancy. Trans Am Soc Artif Intern Organs. 1976;22:80–93. - PubMed
-
- Barbaro RP, Boonstra PS, Moler FW, Davis MM, Prosser LA. Hospital-level variation in inpatient cost among children receiving extracorporeal membrane oxygenation. Perfusion. 2017;32:538–546. - PubMed
-
- Colvin M, Smith JM, Skeans MA, Edwards LB, Uccellini K, Snyder JJ, et al. OPTN/SRTR 2015 annual data report: heart. Am J Transplant. 2017;17:286–356. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
