

Association of thrombocytosis with COPD morbidity: the SPIROMICS and COPDGene cohorts
- PMID: 29373977
- PMCID: PMC5787242
- DOI: 10.1186/s12931-018-0717-z
Association of thrombocytosis with COPD morbidity: the SPIROMICS and COPDGene cohorts
Abstract
Background: Thrombocytosis has been associated with COPD prevalence and increased all-cause mortality in patients with acute exacerbation of COPD (AECOPD); but whether it is associated with morbidity in stable COPD is unknown. This study aims to determine the association of thrombocytosis with COPD morbidity including reported AECOPD, respiratory symptoms and exercise capacity.
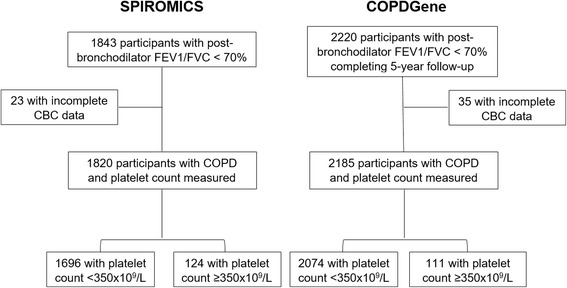
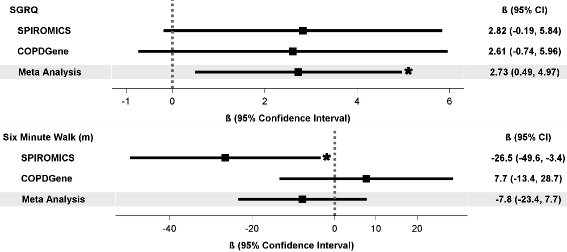
Methods: Participants with COPD were included from two multi-center observational studies (SPIROMICS and COPDGene). Cross-sectional associations of thrombocytosis (platelet count ≥350 × 109/L) with AECOPD during prior year (none vs. any), exertional dyspnea (modified Medical Research Council (mMRC) score ≥ 2), COPD Assessment Test (CAT) score ≥ 10, six-minute-walk distance (6MWD), and St. George Respiratory questionnaire (SGRQ) were modeled using multivariable logistic or linear regression. A pooled effect estimate for thrombocytosis was produced using meta-analysis of data from both studies.
Results: Thrombocytosis was present in 124/1820 (6.8%) SPIROMICS participants and 111/2185 (5.1%) COPDGene participants. In meta-analysis thrombocytosis was associated with any AECOPD (adjusted odds ratio [aOR] 1.5; 95% confidence interval [95% CI]: 1.1-2.0), severe AECOPD (aOR 1.5; 95% CI: 1.1-2.2), dyspnea (mMRC ≥ 2 aOR 1.4; 95% CI: 1.0-1.9), respiratory symptoms (CAT ≥ 10 aOR 1.6; 95% CI: 1.1-2.4), and higher SGRQ score (β 2.7; 95% CI: 0.5, 5). Thrombocytosis was also associated with classification into Global Initiative for Chronic Obstructive Lung Disease (GOLD) group D (aOR 1.7 95% CI: 1.2-2.4).
Conclusions: Thrombocytosis was associated with higher likelihood of prior exacerbation and worse symptoms. Platelet count, a commonly measured clinical assay, may be a biomarker for moderate-severe COPD symptoms, guide disease classification and intensity of treatment. Future longitudinal studies investigating the role of platelets in COPD progression may be warranted.
Trial registration: ClinicalTrials.gov: NCT01969344 (SPIROMICS) and NCT00608764 (COPDGene).
Keywords: Dyspnea; Exacerbations; Platelet count; Quality of life.
Conflict of interest statement
Ethics approval and consent to participate
SPIROMICS and COPDGene were approved by the institutional review boards at each center and all participants provided written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
Associated data
Grants and funding
- P50 MD010431/MD/NIMHD NIH HHS/United States
- R01 HL089897/HL/NHLBI NIH HHS/United States
- HHSN268200900019C/HL/NHLBI NIH HHS/United States
- K23 ES025781/ES/NIEHS NIH HHS/United States
- G12 MD007597/MD/NIMHD NIH HHS/United States
- P30 ES005605/ES/NIEHS NIH HHS/United States
- T32HL007534/HL/NHLBI NIH HHS/United States
- U01 HL089897/HL/NHLBI NIH HHS/United States
- R01HL089897, R01HL089856/HL/NHLBI NIH HHS/United States
- K24 HL137013/HL/NHLBI NIH HHS/United States
- R01 HL089856/HL/NHLBI NIH HHS/United States
- U01 HL089856/HL/NHLBI NIH HHS/United States
- HHSN268200900015C/HL/NHLBI NIH HHS/United States
- HHSN268200900013C, HHSN268200900014C, HHSN268200900015C, HHSN268200900016C, HHSN268200900017C, HHSN268200900018C, HHSN268200900019C, HHSN268200900020C/HL/NHLBI NIH HHS/United States
- HHSN268200900016C/HL/NHLBI NIH HHS/United States
- K23 HL123594/HL/NHLBI NIH HHS/United States
- U01 HL137880/HL/NHLBI NIH HHS/United States
- HHSN268200900018C/HL/NHLBI NIH HHS/United States
- HHSN268200900017C/HL/NHLBI NIH HHS/United States
- HHSN268200900020C/HL/NHLBI NIH HHS/United States
- HHSN268200900013C/HL/NHLBI NIH HHS/United States
- K23 HL130627/HL/NHLBI NIH HHS/United States
- HHSN268200900014C/HL/NHLBI NIH HHS/United States
- K24 HL138188/HL/NHLBI NIH HHS/United States
- T32 HL007534/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
