

Amiodarone Protocol Provides Cost-Effective Reduction in Postoperative Atrial Fibrillation
- PMID: 29374511
- PMCID: PMC5963994
- DOI: 10.1016/j.athoracsur.2017.12.029
Amiodarone Protocol Provides Cost-Effective Reduction in Postoperative Atrial Fibrillation
Abstract
Background: Postoperative atrial fibrillation (POAF) after cardiac operations results in a significant increase in morbidity, mortality, and health care costs. Prophylactic amiodarone has been shown to reduce the incidence of POAF; however, the cost-effectiveness of a protocol-driven approach remains unknown.
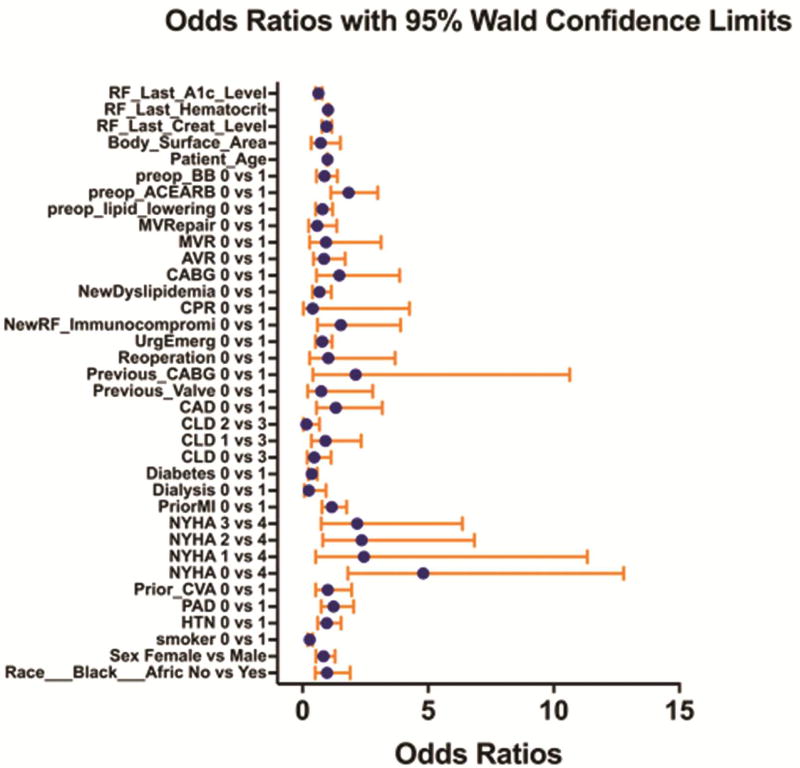
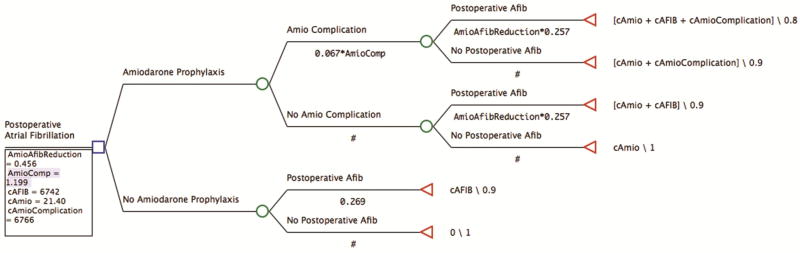
Methods: All patients with a Society of Thoracic Surgeons risk score enrolled in a prophylactic amiodarone protocol (n = 153) were propensity score matched 1:3 with patients before protocol implementation (n = 3,574). Multivariate logistic and linear regressions assessed the relative risks (POAF reduction and adverse medication effects) in the matched cohort of amiodarone therapy and costs, respectively. TreeAge cost-effectiveness software (TreeAge Software, Inc, Williamstown, MA) modeled the effects of prophylactic amiodarone costs, complication rates, and quality of life.
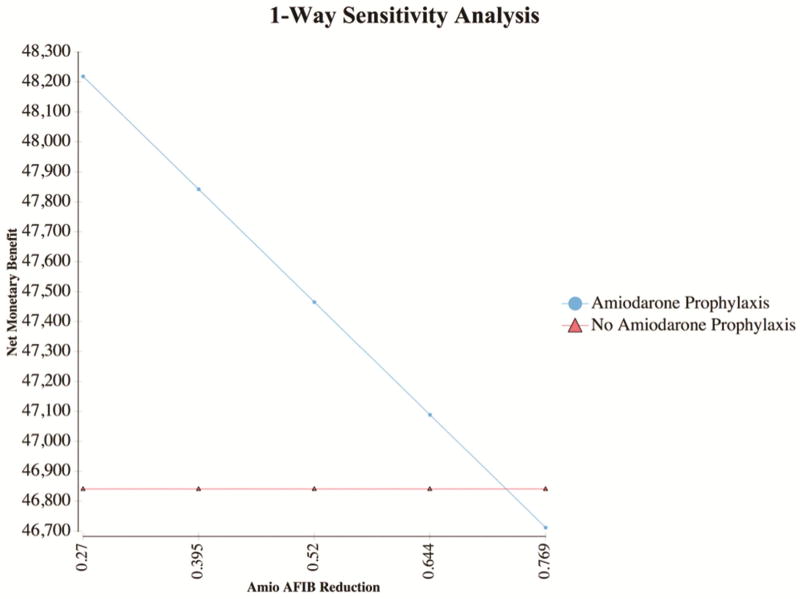
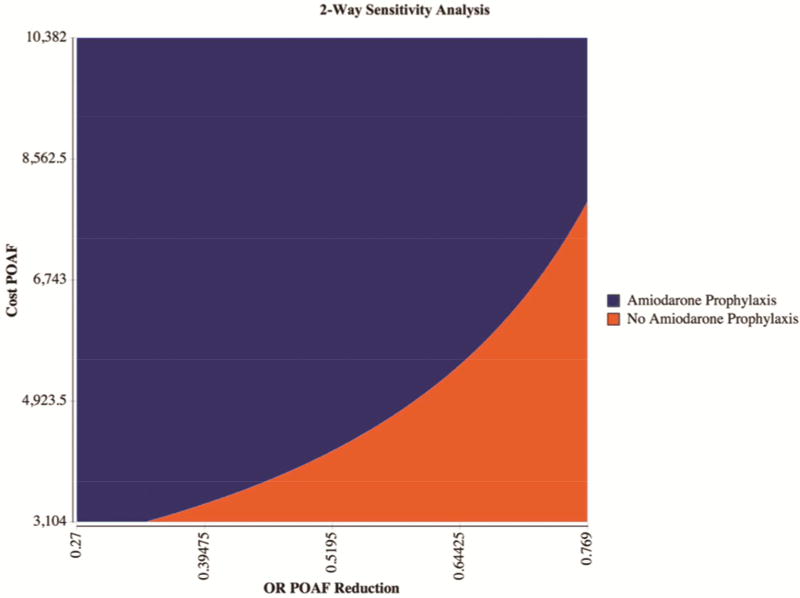
Results: Of patients eligible for the prophylactic amiodarone protocol, 94.3% (281 of 298) were enrolled. Prophylactic amiodarone significantly reduced the rate of POAF (25.7% vs 16.8%, p < 0.0001). A total of 600 matched patients demonstrate no baseline differences in demographics, comorbidities, disease state, or operative factors, with a significant reduction in POAF without an increase in other associated complications. With the use these adjusted estimates, the prophylactic amiodarone protocol demonstrated a cost savings of $458 per patient. Sensitivity analysis confirmed the protocol is cost-effective for all protocol-related POAF risk reductions below an odds ratio of 0.726.
Conclusions: Implementation of a prophylactic amiodarone protocol significantly reduced risk-adjusted rates of POAF, with a cost savings of $458 per patient. This analysis demonstrates how rigorous quantitative analysis can evaluate the benefits of quality improvement projects.
Copyright © 2018 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Invited Commentary.Ann Thorac Surg. 2018 Jun;105(6):1702-1703. doi: 10.1016/j.athoracsur.2018.01.062. Epub 2018 Mar 6. Ann Thorac Surg. 2018. PMID: 29501654 No abstract available.
-
Prophylaxis with amiodarone for postoperative atrial fibrillation: when and who?J Thorac Dis. 2018 Nov;10(Suppl 33):S3831-S3833. doi: 10.21037/jtd.2018.10.14. J Thorac Dis. 2018. PMID: 30631490 Free PMC article. No abstract available.
References
-
- Maisel WH, Rawn JD, Stevenson WG. Atrial fibrillation after cardiac surgery. Annals of internal medicine. 2001;135(12):1061–1073. - PubMed
-
- Almassi GH, Pecsi SA, Collins JF, Shroyer AL, Zenati MA, Grover FL. Predictors and impact of postoperative atrial fibrillation on patients' outcomes: A report from the randomized on versus off bypass trial. The Journal of thoracic and cardiovascular surgery. 2012;143(1):93–102. - PubMed
-
- Bramer S, van Straten AH, Soliman Hamad MA, Berreklouw E, Martens EJ, Maessen JG. The impact of new-onset postoperative atrial fibrillation on mortality after coronary artery bypass grafting. The Annals of thoracic surgery. 2010;90(2):443–449. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
